
Shoulder Ultrasound
by Pierre Vassallo
Ultrasound (US) has been shown to be an effective imaging modality in the evaluation of both rotator cuff and non–rotator cuff disorders. Magnetic resonance imaging has taken on a secondary role in shoulder imaging for assessing sonographically inaccessible structures such as bone, labral cartilage, deep parts of various ligaments, capsule, and areas obscured by bone.
Ultrasound has several advantages over MRI for shoulder imaging. Ultrasound is a quick and inexpensive technique that is more widely and readily available. Ultrasound also has a higher spatial resolution than MRI and therefore has the potential of demonstrating smaller details (MRI has a higher contrast resolution). Ultrasound allows dynamic assessment of moving structures and can better assess problems such as tendon impingement and tendon subluxation (particularly of the long head of biceps tendon). Ultrasound allows the examiner to go directly to the site of pain as indicated by the patient so that the structure and often the pathological process causing the symptoms can be immediately identified. Ultrasound is also very effective for guiding interventions such as steroid infiltrations, fluid aspirations and aspiration of liquid calcific deposits. Tendon calcifications are best seen with ultrasound (they are not visible on MRI). Ultrasound may be the only option in patients with metallic implants in the shoulder and pacemakers as well as in claustrophobic patients who will not tolerate an MRI scan. The following paragraphs will outline the most common types of pathology affecting rotator cuff and non-rotator cuff structures and their appearances on ultrasound.

Figure 1. The rotator cuff tendons encircle the humeral head to retain it in the glenoid fossa. The long head of biceps tendon passes between the subscapularis and supraspinatus tendons.
The rotator cuff is composed of four tendons that are fused together to form a supporting sleeve to stabilise the humeral head within the shallow glenoid fossa. The Medical Imaging Figure 1. The rotator cuff tendons encircle the humeral head to retain it in the glenoid fossa. The long head of biceps tendon passes between the subscapularis and supraspinatus tendons. tendons include from posterior to anterior, the teres minor, the infraspinatus, the supraspinatus and the subscapularis tendons (Figure 1).
A small gap between the subscapularis and supraspinatus tendons allows the passage of the long head of biceps tendon; this is called the rotator cuff interval.
The supraspinatus tendon is the tendon most commonly involved in rotator cuff disease. Since the supraspinatus runs above the humeral head and below the acromion of the scapula, it is prone to impingement in this restricted location. Also it is the most superiorly located tendon of the cuff and therefore takes most of the load particularly during arm abduction. The supraspinatus tendon is seen on ultrasound as an echogenic band exiting below the acromion and tapering towards its attachment into the greater humeral tuberosity. It frequently shows a fibrillar pattern (fine longitudinal lines within it) and close to attachment (due to reflection of sound waves by the parallel running fibers) a dark area may be seen which is called anisotropy and is normal (Figure 2).
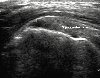
Figure 2. Supraspinatus tendon in longitudinal view is seen as an echogenic band superior to the humeral head, with a convex upper surface that tapers toward the greater tuberosity. The arrow indicates a hypoechogenic area due to tendon anisotropy (arrow).
Supraspinatus tendon degeneration also known as supraspinatus tendonosis is the result of repeated strain injury and impingement of the supraspinatus tendon. A longitudinal scan through the tendon shows thickening of the tendon and hyperechogenicity due to deposits of myxoamatous tissue (Figure 3). Supraspinatus tendonopathy may also present with calcifications within the tendon (Figure 4).
Calcific tendinitis is a common disorder caused by deposition of calcium hydroxyapatite crystals. The cause is considered to be dystrophic, and all tendons can be affected, although the most common site is within the supraspinatus tendon near its insertion. A partial-thickness supraspinatus tendon tear extends either to the articular or bursal surface of the tendon. An articular-side partial-thickness tear appears as a distinct hypoechoic or mixed hyper-hypoechoic defect of the articular surface (Figure 5). A bursal-side partialthickness tear produces flattening of the bursal surface, with loss of the superior convexity of the tendon (Figure 6).
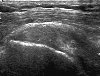
Figure 3. A longitudinal view of the supraspinatus tendon demonstrates a heterogeneous echogenicity in the tendon without any tendon gap. This pattern may compatible with tendinosis.

Figure 4. A longitudinal view showing two dense calcifications (c) with posterior shadowing near the insertion of the supraspinatus tendon.
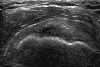
Figure 5. A longitudinal view of the supraspinatus tendon shows a partial-thickness tear as a distinct hypoechoic defect (arrow) at the tendon’s articular side.
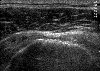
Figure 6. A transverse view of the supraspinatus tendon showing a partial-thickness bursal side tear; note the flattening (T) of the normally convex superior margin of the supraspinatus tendon.

Figure 7. A longitudinal view of the supraspinatus tendon showing a full-thickness tear (T) filled with anechoic joint fluid.
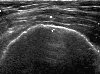
Figure 8. A longitudinal view of the supraspinatus tendon shows a complete tear of the tendon; the tendon absent and the deltoid muscle (D) is now in contact with the humeral head (H).
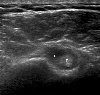
Figure 9. Transverse view of the biceps tendon (T) showing hypoechoic fluid collection within the tendon sheath (F)
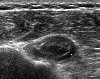
Figure 10. A transverse view of the LHBT shows an enlarged tendon (T) with an inhomogeneous echotexture and associated fluid in the sheath (F) that are features of tendinosis.
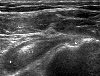
Figure 11. Transverse view through the bicipital groove shows a subluxed LHBT (BT) is surrounded by a hypoechoic fluid.

Figure 12. Steroid infiltration of the subdeltoid bursa with realtime control of needle (N) entering the subdeltoid bursa (S) from the left.
A full-thickness tear of the supraspinatus tendon presents with a gap involving the full thickness of the tendon that is filled with fluid or debris (Figure 7). A complete tear of the supraspinatus tendon presents with absence of the tendon below the deltoid muscle (Figure 8).
Due to the complete tear, the supraspinatus tendon has retracted medially and as a result, the deltoid muscle is now in contact with the humeral head. The long head of biceps tendon is the also commonly involved in acute or chronic shoulder injuries. The most common finding is rotator cuff tenosynovitis that present with fluid in the tendon sheath (Figure 9).
Long head of biceps tendonosis may also occur and present with a thickened, heterogeneous and hypoechoic tendon (Figure 10). Long head of biceps subluxation out of the bicepital groove may result from trauma and is readily diagnosed by ultrasound particularly during dynamic internal and external rotation of the arm (Figure 11).
Finally, ultrasound is also used to guide interventional procedures, particularly steroid infiltrations and aspiration of fluid collections. The real-time monitoring of these procedures with ultrasound ensures accurate delivery of medication and confirmation of completeness of fluid aspiration (Figure 12).
High-resolution US has proved to be an efficient imaging modality for the assessment of a wide spectrum of rotator cuff and non–rotator cuff disorders, the more common of which have been described above. It is fast and inexpensive and allows dynamic assessment of the joint. A direct correlation of the imaging findings with the patient symptoms can be easily obtained and interventional procedures can be guided.