Recent Advances in Cardiovascular Imaging – Part I
Andrew Borg
Cardiovascular imaging as a subspecialty field within the mother specialties of Cardiology and Radiology has become increasingly popular over the last decade. The main reasons behind this are (a) the rapidly expanding repertoire of imaging modalities, as seen with the advent of cardiovascular magnetic resonance imaging (CMR) and cardiac computed tomography (CCT), (b) the technological improvements which greatly improve the reliability of these examinations, exemplified by rapid tomographic scanning, real time 3D echocardiography and the introduction of ultrasonic contrast agents, and (c) the potential to reduce the need for invasive investigations, represented mainly by the wide choice of functional imaging modalities to detect cardiac ischaemia, and the tissue characterisation potential of CMR.
In this review, I will summarise the technological advances in cardiovascular imaging, highlighting their important clinical role. The first part of this series will deal with echocardiography, while the second part will address the role of cardiac tomographic imaging (Computed tomography and Magnetic Resonance Imaging).
Contrast Echocardiography
An important technical innovation is the introduction of intravenous sonographic contrast. This is a non-iodinecontaining emulsion of inert gas microbubbles encapsulated in an albumin or lipid shell, which oscillate when exposed to ultrasound, producing a strong acoustic backscattered signal. Injection of this contrast, which is very safe, highly enhances the contrast between the blood pool and the myocardium. This vastly improves the diagnostic quality, especially in patients with poor ultrasound penetration. An interesting offshoot of this technology is the use of the rate of replenishment of myocardium with contrast to assess myocardial perfusion in the assessment of suspected ischaemic heart disease. In the future, specially designed microbubbles with specific ligands attached to their shells may be used to image diseased tissue or even deliver drugs and genetic material to the targeted tissue.
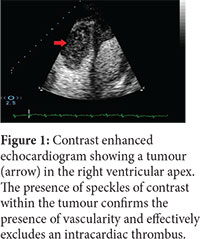
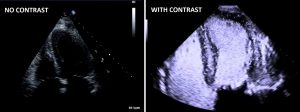
The main role of contrast echocardiography is to diagnose the nature of structures within the heart which are difficult to visualise on non-enhanced scanning. Common examples are intramural thrombi, benign trabeculations and the prominent trabeculations of non-compaction cardiomyopathy, intracardiac tumours (figure 1), the localised myocardial thickening of hypertrophic cardiomyopathy and visualisation of the right ventricle in suspected arrhythmogenic right ventricular cardiomyopathy. Contrast is often used simply to enhance the endocardial lining to facilitate quantification of left ventricular function (figure 2). Finally, the use of intravenous contrast has immensely increased the feasibility and diagnostic potential of stress echocardiography.
Stress Echocardiography
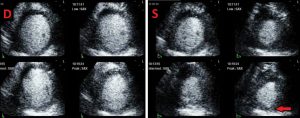
The main use of this technology is in the diagnosis of cardiac ischaemia in patients with chest pain. This modality is based on assessing the contractile response to inotropic drugs (dobutamine), vasodilators (dipyridamole or adenosine) or exercise stress (bicycle or treadmill). Typically, ischaemic segments manifest decreased and delayed systolic thickening at high levels of inotropic stress (figure 3). Such a response has been shown to be highly accurate in detecting significant coronary stenosis and providing prognostic information on the likelihood of cardiac events, with a performance similar to other functional imaging modalities such as nuclear imaging. Whereas the technology has been previously limited by technical problems in visualising all segments of the heart muscle, the use of contrast has eliminated this problem in more than 95% of heart segments, and significantly increased accuracy in the detection of coronary stenosis. Thus, this cheap, versatile and safe modality is considered to be one of the first line investigations for the diagnosis of suspected ischaemia in patients with moderate likelihood of coronary artery disease. Finally, routine indications for stress echocardiography have, over the years, extended beyond the diagnosis of coronary artery disease to include assessment of myocardial viability, valve disease, hypertrophic cardiomyopathy and diastolic function.
3D Echocardiography
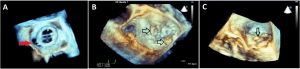
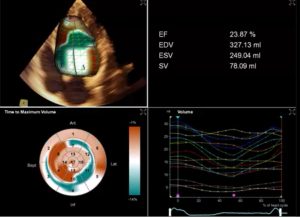
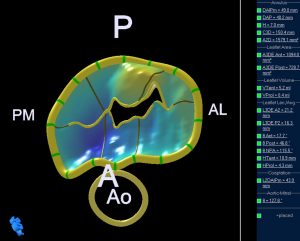
Probably the most impressive development in image acquisition and processing is 3D echocardiography. Whereas previously an experienced cardiologist had to mentally reconstruct a 3D appreciation of a structure from a series of strategically acquired 2D images, modern transducers are capable of acquiring a 3D pyramidal-shaped block of data, allowing real-time visualisation of cardiac structures and their complex spatial relation with neighbouring structures. The high resolution images obtained by transoesophageal imaging (by virtue of the proximity of the probe to the structures being interrogated, allowing the use of a higher frequency probe) lend themselves nicely to 3D reconstruction, generating images which have revolutionised the approach towards heart disease. This has proved indispensable in assessing valvular heart disease (figure 4), measuring ventricular volumes (figure 5), and guiding percutaneous cardiac procedures. Providing a 3D view of a complex three-dimensional structure such as the regurgitant mitral valve facilitates communication with the surgeon (the imager can literally see what the surgeon sees) and facilitates the appreciation of disease by less experienced operators (figure 4). Complex 3D structures such as the mitral valve annulus can be quantified with commercially available software, leading to highly informative models (figure 6). There is no doubt that such models prove indispensable for understanding the mechanism of disease and guiding surgical intervention.
Conclusion
Echocardiography is a well-established technique, with the main advantages being its low cost, portability and lack of ionising radiation. However, ultrasound physics places some inevitable constraints on the technology. Some patients have poor image quality, and unusual cardiac anatomy can prove difficult to quantify, regardless of the operator expertise. Some structures are beyond ultrasonic interrogation, either because they lie behind bone (like the right ventricle in some patients), behind air-containing organs (such as the ascending and descending aorta) or simply because they are too far away from the transducer (as in obese patients). The use of intravenous contrast has gone a long way in improving image quality in challenging patients, but there will always be physical limits to ultrasound propagation in tissue, no matter how advanced the computing power at hand. This is where tomographic imaging, the topic of the next review, enters the scene.