
An Update in Breast Cancer Epidemiology and Healthcare Services in Malta
Jason Attard, Miriam Dalmas & Kathleen England
Abstract
Cancer of the breast is the most common malignancy and the leading cause of cancer-related mortality in women. Over the past 20 years, mortality from breast cancer in Malta has shown a steady decline and survival from this disease has registered marked improvement, despite the fact that incidence continues to increase. Increased awareness as well as the development of specialized breast care health services have resulted in positive outcomes, with local mortality rates approaching that of the EU-15 average.
Background
Breast cancer is the most common malignancy in women accounting for about one quarter of all female cancers and is the leading cause of cancer-related mortality in women.1 On average, 57% of breast cancer cases are diagnosed in women below the age of 65 years.2 The average 5-year relative survival of European women diagnosed with breast cancer in 1999-2007 was 81.8 (95% confidence interval: 81.6-82.0).2
The risk of breast cancer is highest in affluent westernised populations.1 The Western lifestyle, characterised by a high-caloric diet, rich in animal fat and proteins, together with low physical activity, has been shown to be associated with an increased risk of breast cancer.3 Women with a higher body mass index are at a higher risk. On the other hand, sustained physical activity throughout the life course protects women by about 20-40%.4 Furthermore, the excessive consumption of alcohol is associated with a mild increase in the risk of breast cancer with risk increasing linearly with increasing intake.5 Also, recent evidence shows a potentially causal relationship between smoking and breast cancer, especially if long-term and heavy and if started at an early age.6
Other risk factors include a family history of breast cancer in first degree relatives, late childbirth, no history of breastfeeding, early menarche and late-onset menopause.7 There is a small increase in the relative risk in women who used combined oral contraception and in those who used hormonal replacement therapy.7
Breast Cancer Epidemiology in Malta
i. Incidence
The Malta National Cancer Registry8 reports that during the time period 2011-2013, the average annual incidence in Malta amounted to 323 cases per year. The average age at diagnosis was 63.4 years and the age range varied from 17 to 97 years.
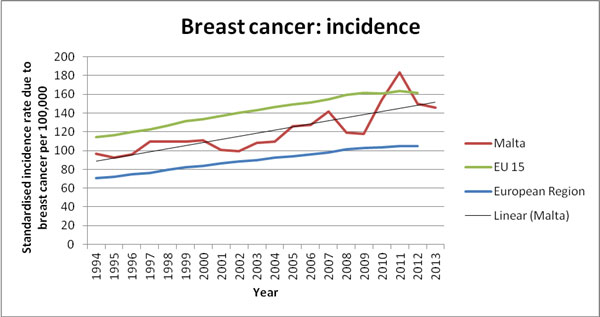
In Malta, the incidence rates of breast cancer have been steadily increasing over the past 20 years. Incidence rates for Malta are lower than the average of the EU 15 Member State countries (EU member states pre-2004 accession), but higher than the average of the European Region countries (53 countries under the remit of the WHO Regional Office for Europe) (figure 1).9 Overall, it is clear that there is a steady upward trend across Europe. Of note, it appears that since 2008, the upward trend for the average EU 15 Member State countries has plateaued (the annual rates show a more flattened pattern).
Figure 1. Breast cancer incidence rate time trends: 1994-2013.9(Annual fluctations in the incidence rate for Malta are often due to small numbers and therefore a linear trend line has been added which depicts the general trend in the incidence rate for Malta).
ii. Mortality
During the time period 2011-2013, the average annual mortality attributed to breast cancer in Malta amounted to 82 deaths. The average age at death from breast cancer was 71.1 years and the age range varied from 31 to 96 years.10
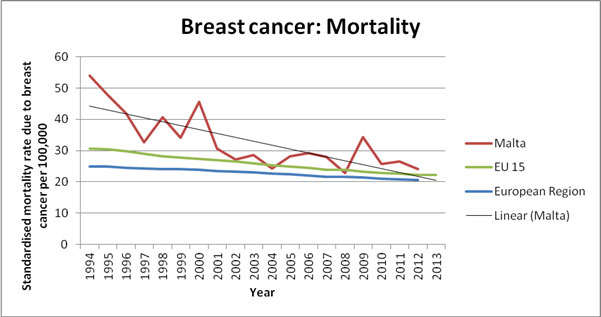
Time trends for the breast cancer mortality rates for Malta have shown a steep decrease over the past 20 years, approaching the average EU 15 mortality rate. The time trends of standardised mortality rates of breast cancer in the European Region, the EU 15 member states, and in Malta are depicted in Figure 2.9 The fall in standardized mortality rate over time is due both to an increase in the age at death and improvements in the overall survival from breast cancer.
Figure 2. Breast cancer mortality rate time trends: 1993-2013.8
iii. Survival
The prognosis of breast cancer depends on the stage at diagnosis, the histological type and tumour grade, the immunophenotype (such as the expression of human epidermal growth factor receptor type 2 and oestrogen/progesterone receptor), and the overall health status of the individual.11 Improvements in survival are the product of health care access, earlier disease detection (for example, through population screening), and advances in treatment. The widespread use of hormonal agents in oestrogen receptor-positive tumours, coupled with effective chemotherapeutic drug regimes have both resulted in a better overall prognsois, including an increase in remission rates and lower recurrence rates.12
In Malta, the 5-year relative survival rate has increased from 75.4 years for women diagnosed in 1990-1994,13 to 75.9 years14 and 84.4 years15 for those diagnosed in 1995-1999 and 2000-2007, respectively. Despite this clear improvement in breast cancer outcomes, the relative survival rate in Malta is still persistently lower than the European average (based on 29 European countries grouped into five European regions).15 This distinction is most discernible when comparing the outcomes for Malta with those of Northern Europe but it is also notable when compared to the average for Southern Europe (see Table 1).
Table 1. Age-specific and age-standardised relative survival for breast cancers diagnosed in 2000-2007, by European region and overall.15
| Age-standardised relative survival with 95% confidence intervals in parentheses | ||||
| Number of cases | 1-year | 5-year | Conditional | |
| Northern Europe | 138,062 | 96.4 (96.2 – 96.5) | 84.7 (84.4 – 85.1) | 87.9 (87.6 – 88.3) |
| Ireland and UK | 364,027 | 93.4 (93.3-93.6) | 79.2 (79.0 – 79.4) | 84.7 (84.5 – 85.0) |
| Central Europe | 318,766 | 95.7 (95.6 – 95.8) | 83.9 (83.6 – 84.1) | 87.7 (87.5 – 87.9) |
|
Southern Europe Malta |
173,693 1,806 |
95.6 (95.4 – 95.7) 95.7 (94.4 – 97.1) |
83.6 (83.3 – 83.9) 80.8 (77.3 – 84.4) |
87.5 (87.2 – 87.8) 84.4 (81.0 – 87.9) |
| Eastern Europe | 121,443 | 91.0 (90.8 – 91.3) | 73.7 (73.2 – 74.1) | 80.9 (80.5 – 81.4) |
| Europe (based on 29 European countries) | 1,115,991 | 94.8 (94.7 – 94.9) | 81.8 (81.6 – 82.0) | 86.3 (86.1 – 86.5) |
In conclusion, over the past 20 years, mortality from breast cancer in Malta has shown a steady decline, survival from this disease has registered unrelenting improvement, whilst incidence continues to increase. Consequently, the national healthcare services have grown and evolved in parallel to meet the rising and diversifying needs of the Maltese population.
National Healthcare services for Breast cancer
The Breast Care Unit service was established in 2000 and is currently housed at Mater Dei Hospital. This Unit caters for the diagnosis and surgical treatment of invasive breast cancer (just over 300 new cases per year), as well as non-malignant breast pathologies. It also offers follow-up services. The cancer care pathways (diagnostic workup and treatment plans) of women diagnosed with breast cancer are discussed at weekly multi-disciplinary team (MDT) meetings. The MDT includes breast cancer surgeons and nurses, pathologists, radiologists, oncologists and managers from the national screening program. The Breast Care Unit was renamed the Agatha Breast Unit in 2015 during celebrations to mark 15 years since its inception. During the celebration program, guidelines for diagnosis, treatment and follow-up, coordinated by the clinic’s surgical professionals, were presented and launched. New surgical techniques such as oncoplastic and immediate reconstruction surgery have been introduced to complement the plastic and reconstruction surgery that were already available.
Breast cancer patients are also offered specialized allied healthcare professional services such as occupational therapy, physiotherapy, as well as the services of clinical psychologists and social workers. Physiotherapists also organize a specialized lymphoedema clinic. A number of publications offering information to clients and patients have also been developed and are distributed by the National Screening Unit, the Agatha Breast Unit and the Sir Anthony Mamo Oncology Centre.
Newer health technologies are improving the diagnostic capabilities across the board. In the medical imaging department, two full-field digital mammography machines with stereo-guided equipment, ultrasound equipment equiped with 2D and 3D probes, and a 3 Tesla MRI scanner with dedicated breast software were introduced. Current pathology services are also increasingly relying on immunohistochemistry to test for oestrogen and progesterone receptors, HER2 amplification and other basal biomarkers. The results of these investigations are allowing a more personalised approach to the adjuvant and neo-adjuvant therapy that can be offered to patients.
Oncological treatments, namely chemotherapy, hormone therapy and radiotherapy, and palliative care are managed and delivered at Sir Anthony Mamo Oncology Centre. . The new Oncology Centre, which was inaugurated in 2015, is equiped with 3 linear accelerators, planning stations and a large bore CT simulator.
Population-based organised mammography screening was introduced towards the end of 2009 for women aged between 50-60 years. By 2015, this has been extended up to women that are 65 years old. In the Health Interview Survey (2008) that was conducted before the introduction of the organised screening program, 40% of women in the 50-65 year group reported that they had at least one mammography in the preceding three years.16 During 2013, the screening program performed mammography screening on 9,027 women (58.1% of the women invited for screening during 2013). Of these, 44 women were eventually referred for further investigation and treatment of breast pathology. The breast pathology of 35 of these women was confirmed to be invasive breast cancer while the remaining 9 cases were eventually confirmed to be carcinoma-in-situ.
Conclusion
The comprehensive breast cancer care services which are offered in Malta, have consistently been shown to be continuously improving. The outcomes of these services can be further improved through initiatives to lower incidence through the promotion of healthier lifestyles, and reduce mortality by advancing earlier detection through health education and population screening.
Improvement of the breast care services offered can be more vigorously channeled towards achieving higher quality of these services such as through the introduction of initiatives to help reduce the waiting times between different phases of the breast cancer care pathways. Additional effort needs to be devoted towards achieving more positive patients’ experience during the diagnostic and therapeutic phases as well as beyond, through the emerging and important themes of rehabilitation and survivorship. The latter two domains are constantly growing in importance and significance in tandem with achievements in cancer survival.
References
1. Lakhani S. WHO classification of tumours of the breast. Lyon: International Agency for Research on Cancer; 2012.
2. Eu-cancer.iarc.fr. EUCAN Factsheets | Breast cancer [Internet]. 2015 [cited 30 December 2015]. Available from: http://eu-cancer.iarc.fr/eucan/CancerOne.aspx?Cancer=46&Gender=2
3. Department of Health (1998). Report on health and social subjects No. 48. Nutritional aspects of the development of cancer. The Stationery Office: Norwich.
4. Iarc.fr. Weight Control and Physical Activity – IARC Handbook of Cancer Prevention Volume 6 [Internet]. 2016 [cited 7 January 2016]. Available from: http://www.iarc.fr/en/publications/pdfs-online/prev/handbook6/
5. Smith-Warner S, Spiegelman D, Yaun S. Alcohol and Breast Cancer. Southern Medical Journal. 1998;91(7):687.
6. Reynolds P. Smoking and breast cancer. J Mammary Gland Biol Neoplasia. 2013;18(1):15-23.
7. McPherson K, Steel C, Dixon J (2000). Breast cancer- epidemiology, risk factors and genetics. British Medical Journal 2000 September 9; 321 (7261): 624-628.
8. Directorate of Health Information and Research. Malta National Cancer Registry https://health.gov.mt/en/dhir/Pages/Registries/cancers.aspx Accessed on the 15th December 2015.
9. World Health Organisation Regional Office for Europe (2015). Health for All Database (HFA-DB). http://data.euro.who.int/hfadb/. Accessed on 15th December 2015.
10. Directorate of Health Information and Research. Malta National Mortality Registry. https://health.gov.mt/en/dhir/Pages/Introduction.aspx. Accessed on the 15th December 2015.
11. Soerjomataram I, Louwman M, Ribot J, Roukema J, Coebergh J. An overview of prognostic factors for long-term survivors of breast cancer. Breast Cancer Res Treat. 2007;107(3):309-330.
12. Youlden D, Cramb S, Dunn N, Muller J, Pyke C, Baade P. The descriptive epidemiology of female breast cancer: An international comparison of screening, incidence, survival and mortality. Cancer Epidemiology. 2012;36(3):237-248.
13. Coleman M. EUROCARE-3 summary: cancer survival in Europe at the end of the 20th century. Annals of Oncology. 2003;14(90005):128v-149.
14. Berrino F, De Angelis R, Sant M, Rosso S, Lasota M, Coebergh J et al. Survival for eight major cancers and all cancers combined for European adults diagnosed in 1995–99: results of the EUROCARE-4 study. The Lancet Oncology. 2007;8(9):773-783.
15. Sant M, Chirlaque Lopez M, Agresti R, Sánchez Pérez M, Holleczek B, Bielska-Lasota M et al. Survival of women with cancers of breast and genital organs in Europe 1999–2007: Results of the EUROCARE-5 study. European Journal of Cancer. 2015;51(15):2191-2205.
16. Directorate of Health Information and Research. Surveys: European Health interview Survey 2008. https://healthcms.gov.mt/en/dhir/Pages/Surveys/eurohealthintervsurvey2008.aspx Accessed on the 15th December 2015.