
Breast MR Imaging in Mammographically Benign-Appearing Breast Lesions
Pierre Vassallo
Breast cancer is the most common malignancy in women. The most common pathologic subtypes of breast cancer originate in the terminal duct lobular unit in either the ducts (ductal carcinoma) or lobules (lobular carcinoma). These subtypes account for 80%–85% of primary breast cancers. The origin of the breast cancer can only be determined by the microscopic appearance of the cancer cells obtained at biopsy.
Usually, breast cancers manifest as irregularly shaped masses, with or without microcalcifications. Therefore, many breast cancers are diagnosed on the basis of these findings at mammography or ultrasonography (US).
Although most well-circumscribed breast lesions are benign, 10%–20% of breast malignancies are also well-circumscribed; these malignant masses include papillary, mucinous, medullary, and metaplastic carcinomas, as well as malignant phyllodes tumors. Such lesions may be difficult to recognize as malignant using conventional imaging modalities such as mammography and US.
MR imaging has been widely used for detecting and assessing breast lesions. MR imaging is sensitive for detecting breast cancers, with a sensitivity as high as 100% for invasive breast cancers, and therefore has emerged as an adjunctive breast imaging modality to mammography and US. MR imaging has limitations in lesion characterization, but it is still useful as an adjunct for differentiating between benign breast lesions and benign-looking breast cancers. It is also useful for evaluating dense breasts.
Papillary Carinomas may be located in a duct or within a cyst and are therefore mostly located in the retroareolar region. The lesions may be in-situ or invasive. On mammography, papillary carcinomas appear as well-defined dense lesions (Fig 1a). On US, intracystic lesions tend to show internal haemorrhage and also contain solid components within the cyst (Fig 1b). The solid component may show hypervascularity on Doppler US. MR imaging will show smooth lesion margins, areas of haemorrhage (fig 1c), cystic fluid (fig 1d), strong contrast enhancement of the rim and solid polypoid components (fig 1e) and a temporal contrast enhancement pattern indicative of malignant disease (fig 1f). Invasive and non-invasive papillary cancers have similar appearances on US, mammography and MR imaging.
Mucinous (or colloid) carcinoma contains large amounts of extracellular extraluminal mucus in direct contact with the stroma. It is more common in elderly women and usually has a good prognosis. Areas of invasive ductal cancer are however often intermixed within these lesions, which makes the prognosis less favorable. Mucinous carcinoma commonly presents as a well-circumscribed round, oval, or lobular mass on mammography (Fig 2a) and US. Mixed cystic and solid components and the presence of posterior acoustic enhancement may be seen at US (Fig 2b). Mucinous carcinoma shows variable signal intensity on T1-weighted MR images, depending on protein concentration within the tumor (Fig 2c), and is homogeneously or heterogeneously hyperintense on T2-weighted images (Fig 2d), which correlates with the large mucinous component at histologic examination. Dynamic contrast enhanced T1 weighted scans show marked early enhancement with washout (as in Fig 1f) or persistent enhancement (as in Fig 2e).
Medullary carcinoma is an uncommon tumor that accounts for less than 5% of all breast cancers. It has been reported to account for 11% of all breast carcinomas diagnosed in women 35 years and younger and has a relatively favorable prognosis. Medullary carcinoma manifests as a round, oval, noncalcified mass with a well-circumscribed margin at mammography (Fig 3a) and as a well-circumscribed hypoechoic lesion with no dorsal enhancement at US (Fig 3b). Medullary carcinomas show marked homogeneous enhancement on MRI (Fig 3c) with a plateau phase (ie no washout) (Fig 3d).
Metaplastic breast carcinoma is regarded as a ductal carcinoma that has undergone metaplasia into a nonglandular growth pattern, including squamous cell, spindle cell, and heterogeneous mesenchymal growth patterns. It is a rare type of cancer accounting for only 1% of cases and presents more commonly after the age of 50 years. Metaplastic carcinoma usually presents as a rapidly growing mass with no axillary lymphadenopathy. It appears as a well circumscribed lesion on mammography (Fig 4a) and US, being hypoechoic or heterogeneous with mixed solid and cystic components on US (Fig 4b). T2-weighted MRI scans demonstrate the lesion as bright due to the cystic components (Fig 4c). On the other hand contrast-enhanced T1-weighted scans show rim enhancement (as cystic components do not enhance) (Fig 4d). A type III enhancement pattern is seen on dynamic MR study (Fig 4e).
Phyllodes tumors are composed of a mixture of epithelial elements and a connective tissue stroma. Most are benign but intermediate and malignant forms also occur. All three forms of phyllodes tumors have a high recurrence rate. On mammography, a phyllodes tumor appears as a large relatively well-circumscribed soft-tissue mass, showing an appearance similar to a fibroadenoma. US shows a solid hypoechoic mass often with cystic areas, the latter being more common in malgnant lesions. T2-weighted MRI scans demonstrate the cystic components, while contrast enhanced T1-weighted MRI shows heterogeneous enhancement (Fig 5a). Dynamic MR studies show a Type III contrast enhancement pattern (Fig 5b).
In summary, a number of malignant lesions have a benign appearance on mammography and US. MR morphology, contrast uptake and dynamic enhancement pattern analysis serve as a valuable adjunct for correct diagnosis in these cases. High T2 signal, strong and rapid contrast uptake with sustained enhancement or early washout are features of malignant disease.
Figure Legends
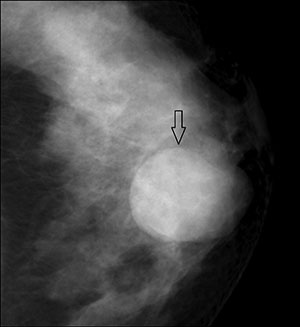
Figure 1a. Mammogram showing an intracystic papillary carcinoma as an oval well-circumscribed high-density mass (arrow).
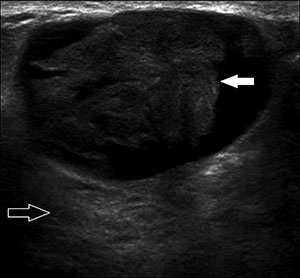
Figure 1b. US demonstrates a solid mass (solid arrow) within a cystic lesion with mild posterior acoustic enhancement (open arrow).
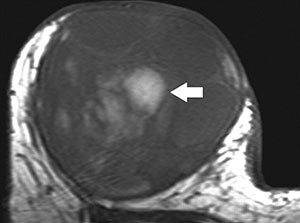
Figure 1c. T1-weighted MR scan of an intracystic papillary carcinoma showing central high T1 signal (bright area) (arrow) within the lesion that is compatible with haemorrhage.
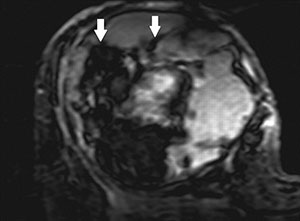
Figure 1d. T2-weighted MR scan of an intracystic papillary carcinoma showing areas of high T1 signal (bright areas) within the lesion compatible with cyst fluid. Black areas (arrows) within the lesion are due to deposits of haemosiderin resulting from older haemorrhage.
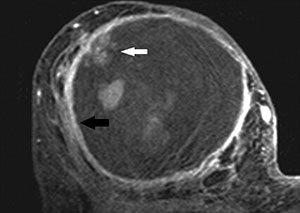
Figure 1e. Axial contrast material–enhanced T1-weighted MR image demonstrates marked enhancement of the cystic wall (black arrow) and mural nodules (white arrow).
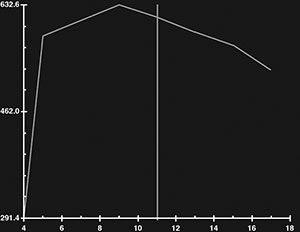
Figure 1f. The dynamic enhancement pattern (signal intensity y axis against time x axis) following (Gadolinium-based) contrast agent injection shows marked early enhancement and also an early washout pattern in the solid portion of the lesion that are features of malignancy (Type III pattern).
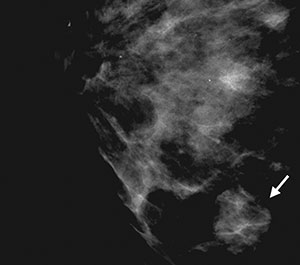
Figure 2a. Mucinous carcinoma on a mammogram shows a lobular well-circumscribed mass lesion (arrow).
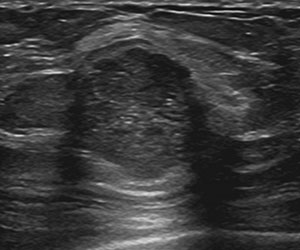
Figure 2b. Mucinous carcinoma on US seen as a round microlobulated mass with posterior acoustic enhancement.
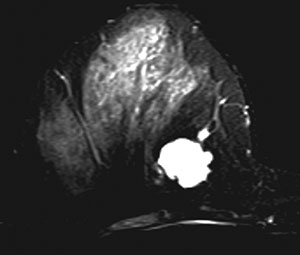
Figure 2c. T2-weighted MR image shows a homogeneously hyperintense lobular mass with a smooth margin.
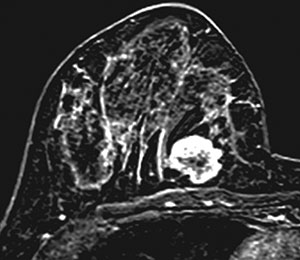
Figure 2d. Contrast-enhanced MR image shows peripheral rim enhancement and an internal nonenhancing portion.
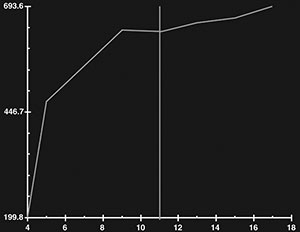
Figure 2e. The dynamic enhancement pattern is the type I persistent pattern
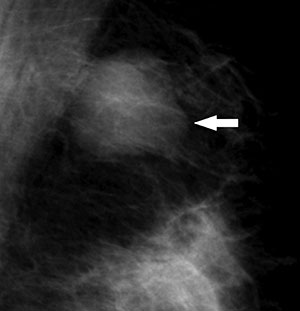
Figure 3a. Medullary carcinoma in a 28-year-old woman presents as a lobular mass (arrow) on mammography.
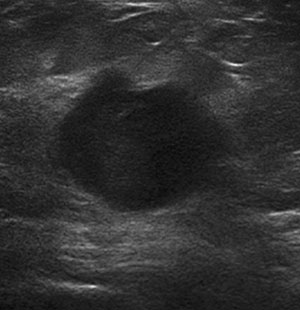
Figure 3b. US of the same lesion shows a lobular hypoechoic mass with a well-defined margins and no dorsal enhancement.
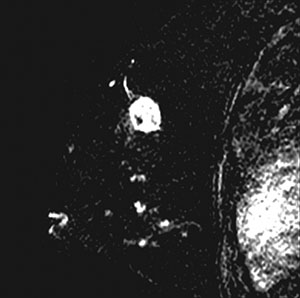
Figure 3c. Medullary carcinoma appears as a rounded well-defined lesion homogeneous contrast enhancement on MRI.
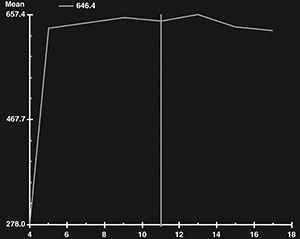
Figure 3d. Dynamic contrast examination shows a type II pattern with rapid and sustained enhancment.
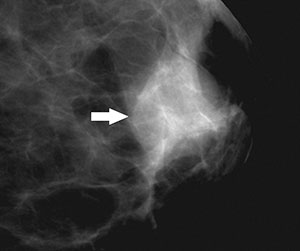
Figure 4a. Focal compression mammography shows a metaplastic carcinoma with mostly well-defined margins (arrow).
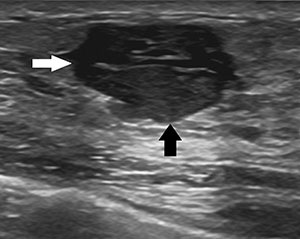
Figure 4b. US shows the same lesion with well-defined margins and heterogeneous internal texture with solid (black arrow) and cystic (white arrow) componements.
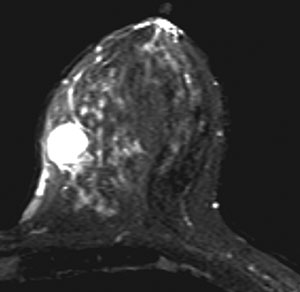
Figure 4c. T2-weighted MRI scan of the same lesion shows high signal due to cystic components.
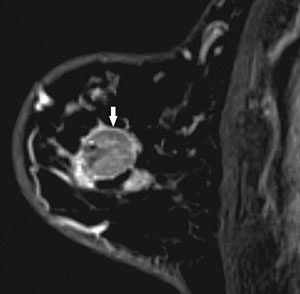
Figure 4d. Contrast enhanced T1-weighted MRI scan shows ring enhancement (arrow) of the lesion.
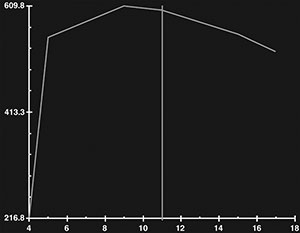
Figure 4e. Dynamic contrast MR study shows a Type III enhancement pattern.
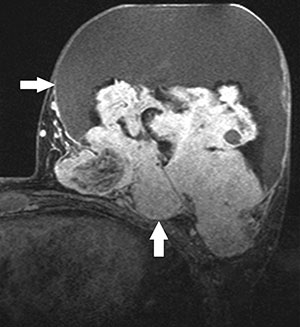
Figure 5a. Contrast-enhanced T1-weighted MRI scan showing heterogeneous enhancement in a phyllodes tumor (arrows).
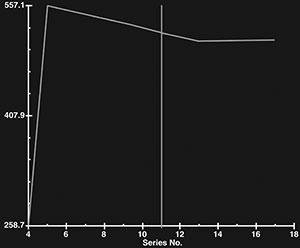
Figure 5b. A type III contrast enhancement pattern is seen in a phyllodes tumor.