
COVID-19 in Malta, a small Island population
Author: Prof Victor Grech
Abstract
Fast tracked. Accepted for publication 24 March 2020
Introduction
Maltese authorities have instituted an escalating series of steps to slow down local COVID-19 infection rates in the hope that the Health Service will not be overwhelmed by the sheer number of severe cases, as witnessed in Northern Italy. This paper will attempt to estimate health effects of COVID-19 on Malta, i.e. infection rates and potential resultant mortality in the absence of effective treatment and/or vaccination. Maximum tolerable infection rates will also be estimated vis-à-vis the expanded intensive care capacities.
Methods
A World Health Organisation report based on the Chinese experience was used.
Results
The local doubling time is 4.9 days and even conservative estimates indicate that the local health services may be overwhelmed.
Discussion
The COVID-19 pandemic is following an approximately exponential curve: it took 67 days to reach the first 100,000 cases, 11 more days to reach 200,000 and just four more to reach 300,000 cases. The weekly admission rates derived in this paper, even with a conservative estimate of a 20% total population infection rate over 14 weeks, would exceed our intensive care ventilation capacity several times over (demand of 281/week as per table 1 versus a supply of 70/week (Malta has a total of approx. 100 ventilators) as per ventilation capacity in results section). Local healthcare risks being plunged into chaos if the public do not do their part. Infection cannot occur in the absence of contact. The only way to mitigate these numbers is to apply social distancing and rigorously apply hand washing, etc.
COVID-19 in Malta, a small Island population.
Introduction
A pandemic is defined as a disease that is prevalent worldwide. While pandemics are known to occur and are planned for,1 it is impossible to predict with any degree of precision when a pandemic (such as an influenza pandemic or the current pandemic COVID-19 pandemic at the time of writing) will strike. These are, by definition, “unknown unknowns; the things we do not yet know that we do not know”,2 so called black-swan situations.3
Coronaviruses
There are four common human coronaviruses in circulation and these account for 10-20% of the common cold cases each year.4 More aggressive coronaviruses have surfaced in the past, strains which acquired the ability to cause severe pneumonias. For example, SARS (Severe Acute Respiratory Syndrome, SARS-CoV) broke out in Asia in 2003 and more than 8,000 people were infected, with a10% mortality.4 MERS (Middle East respiratory syndrome, MERS-CoV) broke out in the Middle East in 2012 and 2,468 were infected with a mortality of >30%.4
COVID-19
The current pandemic is caused by a novel coronavirus (COVID-19, more formally SARS-CoV-2).5 This broke out in December 2019 in Wuhan, China.5,6 The strain is highly contagious with an R0 of ≥3 and a propensity for family clusters. Severity is associated with increasing age and co-morbidities.7 The doubling time is one week or less, so that unchecked, populations rapidly reach 60-80% infection rates.7 It is naturally difficult to estimate precise rates as quite a few individuals are infected and remain asymptomatic (especially children) but are contagious.7 For this reason, unless large proportions of populations are tested continuously, in the absence of a test confirming previous infection, precise denominator data will remain uncertain, introducing wide confidence intervals in any estimate.8
Malta
Malta is one of the smallest countries in the world and comprises a small archipelago in the centre of the Mediterranean Sea with a total population of circa 492,000, a land area of 316 km² and the 7th highest population density in the world. There is only one hospital with intensive care facilities (Mater Dei Hospital) along with a few other smaller facilities and private hospitals.
The Government of Malta, in conjunction with the Health Division and Public Health, have instituted an escalating series of steps that attempt to slow down COVID-19 infection rates in the hope that the Health Service will not be overwhelmed by the sheer number of severe cases, as was the case in Northern Italy in recent days.9 In Malta, schools have closed, social distancing is being strongly advocated and the latest escalation included the closure of non-essential retail outlets and the closure of outlets providing non-essential services.10 These shops may still sell online and deliver their products and fines of €3000 will be imposed for each infraction. The official notice fittingly concludes “These decisions are necessary for the current stage of Covid-19 in Malta and aimed at safeguarding the health of the general public. Co-operation is in the best interest of all.”10
Cognisant of the propensity of COVID-19 to cause severe pneumonias, the country escalated its intensive care ventilator capacity from 20 to potentially 100. In addition, the hospital has been geared to accept 600 COVID-19 cases, a dermatology and cancer hospital (Boffa Hospital) has 12 COVID-19 beds which may be increased to 65, 28 isolation beds are available in another hospital and 120 beds are being prepared in another facility.
This paper will attempt to estimate the health effects of COVID-19 on Malta, i.e. infection rates and potential resultant mortality in the absence of effective treatment and/or vaccination. Maximum tolerable infections rates will also be estimated vis-à-vis expanded intensive care capacities.
Methods
A World Health Organisation report10 based on the Chinese experience estimated that circa:
- 14% of infected cases are severe and require hospitalisation.
- 5% of infected cases are very severe and require intensive care admission, mostly for ventilation (mean length of stay in intensive care is 10 days11)
- 2-4% of infected die.10
Results
Service requirements
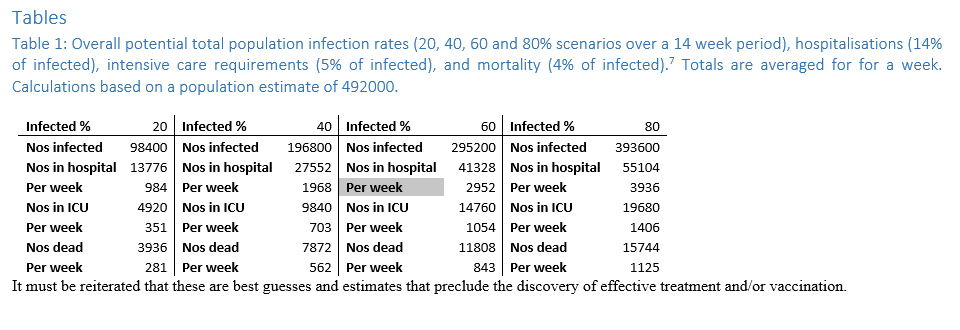
Table 1 displays overall total potential population infection rates (20, 40, 60 and 80% scenarios over a 14 week period), hospitalisations (14% of infected),10 intensive care requirements (5% of infected),10 and mortality (4% of infected).10 Totals are averaged for a week and calculations are based on a population estimate of 492,000.
Infection rate
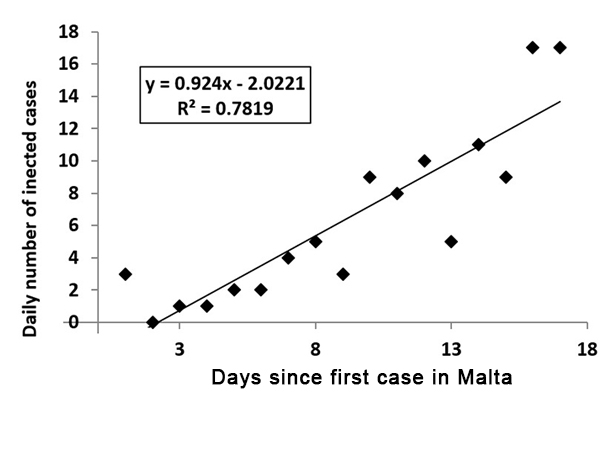
Figure 1 shows a simple graph of daily cases to date. There has only been one severe case requiring hospital admission and no deaths. A simple linear regression model shows reasonable fit (Cases= -2.02+0.92 × Day, adjusted R2= 0.77, p<0.0001). The doubling time is 4.9 days.
Ventilation capacity
Assuming infections continue to increase (whatever the rate, which may be greater or less than that suggested by the above equation), with patients requiring ventilation in a steady state situation, if mean length of stay on ventilator is 10 days, and 100 ventilators are available and fully utilised, then each day, 10 patients need to come off ventilation (recovery or death). Since intensive care cases represent 5% of total infections, a simple proportion calculation shows that if local rates are as quoted by WHO and the Imperial College Report,10,11 when daily infections exceed 200, there will not be enough ventilators to cope with demand, which will exceed 10 daily intensive care admissions daily i.e. more than 70 new ventilator cases per week.
Discussion
The current COVID-19 pandemic is following an exponential curve. Tedros Adhanom Ghebreyesus, Director-General of WHO stated (at a press conference on 23/03/2020 in Geneva) that it took 67 days to reach the first 100,000 cases, 11 more days to reach 200,000 and just four more days to reach 300,000 cases. He noted that this is “heartbreaking. The pandemic is accelerating.”
Actuarial calculations have noted that if Malta were to emulate the trajectory of other countries from day 15, the country would have 2,304 cases by the end of March, and even a 2% fatality rate would result in a hundred deaths by Easter.12
The weekly admission rates derived in this paper, even with a conservative estimate of 20% total population infection rate over 14 weeks, would exceed our intensive care ventilation capacity several times over (demand of 281/week per week as per table 1 versus a supply of 70/week as per ventilation capacity in results section). This calculation assumes that the 100 available ventilator beds are dedicated to COVID-19 patients, a patently optimistic assumption since a significant proportion of the original 20 beds will continue to be needed for other intensive care situations.
Draconian containment measures in China have reduced new cases by more than 90% but this has not been the case elsewhere.9 Italy has been severely affected with the number of infects since February following an exponential trend.9 The events witnessed in Bergamo and Lombardy in the last few days have stunned the global medical community. Intensive care units have been overwhelmed, with the bottleneck being availability of ventilators to tide critically ill patients over their intensive care stay.9 If this region, one of the most affluent parts of Europe, with an advanced healthcare system, was inundated, then it simply cannot be excluded that in chaotic situations wherein cases precipitate suddenly, hospitals (including Mater Dei) may simply collapse and the simple provision of basic care may fail. Other countries are equally besieged.
London is a COVID-19 epicentre which has led to the declaration of total lockdown on 23/03/2020.13 Prime Minister Boris Johnson informed the public in a televised address:
From this evening I must give the British people a very simple instruction — you must stay at home … Without a huge national effort to halt the growth of this virus, there will come a moment when no health service in the world could possibly cope; because there won’t be enough ventilators, enough intensive care beds, enough doctors and nurses … To put it simply, if too many people become seriously unwell at one time, the NHS will be unable to handle it, meaning more people are likely to die, not just from coronavirus but from other illnesses as well.13
Spain and France are also on lockdown as COVID-19 continues to spread rapidly, with Spanish hospitals starting to approach levels witnessed in Northern Italy a few days ago.14 Spread is also widespread in many parts of the United States, with New York considered an epicentre.15
This had led to suggestions that multiple patients could be ventilated with one machine, effectively multiplying intensive care capacity to deal with such “surges”.16 However, this is no solution and the careful application of basic containment measures in order to “flatten the curve”11 cannot be overestimated: hand washing with soap and water, avoiding touching the face and social distancing – staying home, avoiding crowds and refraining from touching one another.7
If these measures are not widely embraced, Malta may witness a spike in cases as happened in Northern Italy, and non-availability of ventilators may lead to triage situations with doctors having to choose who to ventilate and who to leave to die.17 If these measures are not embraced on a global scale, in the absence of effective treatment and/or vaccination, the world may witness catastrophic levels of mortality of circa a quarter of a billion deaths (4%) of the global population.18
Witnessing the events unfolding in March 2020 is almost as if we are witnessing a dystopian science-fiction narrative of the most ghastly kind, with no way out of this unfolding human tragedy. Sadly, despite the fact that this scenario has been modelled worldwide by epidemiologists and depicted in many science fiction narratives,19 we have failed to use this foresight to adequately gird ourselves for such a struggle.
Conclusion
At the risk of sounding melodramatic, but with an extreme sense of realism, healthcare risks being plunged into chaos if the public do not do their part. The Maltese Public Health and National Health Services are doing their upmost, to the extent of initiating the construction of a prefabricated hospital in eight weeks.20 However, the old saw is very applicable: prevention is far better than cure, and infection cannot occur in the absence of contact. The only way to mitigate these numbers is to apply social distancing and take the precautions outlined above.
References
- Fehr AR, Perlman S. Coronaviruses: an overview of their replication and pathogenesis. Methods Mol Biol. 2015;1282:1–23. doi:10.1007/978-1-4939-2438-7_1
- Knight FR. Risk, uncertainty and profit. New York: Houghton-Mifflin Co, 1921.
- Taleb NN. Antifragile: things that gain from disorder. London: Penguin, 2013.
- Yin Y, Wunderink RG. MERS, SARS and other coronaviruses as causes of pneumonia. Respirology. 2018;23(2):130–137. doi:10.1111/resp.13196
- Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
- Ding Q, Lu P, Fan Y, Xia Y, Liu M. The clinical characteristics of pneumonia patients co-infected with 2019 novel coronavirus and influenza virus in Wuhan, China [published online ahead of print, 2020 Mar 20]. J Med Virol. 2020;10.1002/jmv.25781. doi:10.1002/jmv.25781
- World Health Organisation. Coronavirus disease 2019. WHO Report 41. 01 March 2020.
- Velavan TP, Meyer CG. The COVID-19 epidemic. Trop Med Int Health. 2020;25(3):278–280. doi:10.1111/tmi.13383
- Remuzzi A, Remuzzi G. COVID-19 and Italy: what next? [published online ahead of print, 2020 Mar 13]. Lancet. 2020;S0140-6736(20)30627-9. doi:10.1016/S0140-6736(20)30627-9
- Office of the Deputy Prime Minister and the Ministry for Health. PR200539. 22/03/2020 https://www.gov.mt/en/Government/DOI/Press%20Releases/Pages/2020/March/22/pr200539en.aspx
- Ferguson NM on behalf of the Imperial College COVID-19 Response Team. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. March 2020, Imperial College. https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf
- Cortis D. Why coronavirus experts fear the worst is yet to come. Times of Malta 23/03/2020. https://timesofmalta.com/articles/view/why-coronavirus-experts-fear-the-worst-is-yet-to-come-dominic-cortis.780164
- Elliott F. Coronavirus: ‘You must stay at home’. Times of London. 24 March 2020. https://www.thetimes.co.uk/edition/news/coronavirus-you-must-stay-at-home-6rjwndr0c
- Bremner C. Spain and France on lockdown as coronavirus spread continues. Sunday Times of London. 15 March 2020. https://www.thetimes.co.uk/article/spain-and-france-on-lockdown-as-coronavirus-spread-continues-xn3cqjzn9
- Rosenthal BM. Density Is New York City’s Big ‘Enemy’ in the Coronavirus Fight. New York Times. 23 March, 2020. https://www.nytimes.com/2020/03/23/nyregion/coronavirus-nyc-crowds-density.html
- Neyman G, Irvin CB. A single ventilator for multiple simulated patients to meet disaster surge. Acad Emerg Med. 2006;13(11):1246–1249. doi:10.1197/j.aem.2006.05.009
- Ayebare RR, Flick R, Okware S, Bodo B, Lamorde M. Adoption of COVID-19 triage strategies for low-income settings [published online ahead of print, 2020 Mar 11]. Lancet Respir Med. 2020;S2213-2600(20)30114-4. doi:10.1016/S2213-2600(20)30114-4
- Grech V. Unknown unknowns – COVID-19 and potential global mortality. Early Hum Dev. – in press.
- McEuen PL. Science fiction: A post-pandemic wilderness. Nature. 2013 Aug 21;500(7463):398.
- Xuereb M. Health ministry seeks to build prefabricated hospital in eight weeks. Times of Malta 24/03/2020. https://timesofmalta.com/articles/view/health-ministry-seeks-to-build-prefabricated-hospital-in-eight-weeks.780581

{kind=link}
{kind=link}