
Imaging complications of Assisted Reproductive Procedures
Pierre Vassallo
The incidence of assisted conception has increased dramatically in Europe, doubling over the past decade. Assisted reproductive technology (ART) is involved in approximately 1% of births in the developed world. With the increasing use of ART, doctors and radiologists are more likely to encounter associated complications that are sometimes life-threatening. These complications include ovarian hyperstimulation syndrome (OHSS), ovarian torsion, and ectopic and heterotopic pregnancy. Awareness of these entities and their imaging features will facilitate accurate and timely diagnosis and help avoid potentially fatal consequences.
OHSS is a potentially life-threatening iatrogenic complication of ovulation induction or ovarian stimulation. It occurs during the luteal phase of the menstrual cycle or in early pregnancy. Its pathogenesis involves secretion of ovarian vasoactive angiogenic substances (vascular endothelial growth factor – VEGF) by the granulosa-lutein cells of the ovary particularly under the influence of hCG, which cause increased capillary permeability and accumulation of fluid in the extravascular space. This manifests with bilateral ovarian enlargement by multiple cysts, third-spacing of fluids (i.e. ascites, pleural effusions and dependent oedema), and clinical findings ranging from gastrointestinal discomfort to life-threatening renal failure and coagulopathy (due to haemoconcentration).
OHSS is classified according to the Golan classification into mild, moderate and severe based on ultrasound and clinical findings (Table 1). The incidence of OHSS varies by stimulation regimen. Clomiphene induction is associated with rates of mild and moderate OHSS of approximately 13.5% and 8%, respectively; the severe form is rarely seen in association with clomiphene induction. Following gonadotropin stimulation (particularly hCG), the incidence of mild, moderate, and severe OHSS is 20–33%, 3–6%, and 0.1–2%, respectively.
| Category | Ovarian size (cm) | Grade | Signs / symptoms |
| Mild | <6cm | I | Abdominal distension |
| II | Abdominal distension, nausea, vomiting, diarrhoea | ||
| Moderate | 6-12cm | III | Abdominal distension, nausea, vomiting, diarrhoea, ascites on US, weight gain |
| Severe | >12cm | IV | Ascites/pleural effusion |
| V | Ascites/pleural effusion, hypovolaemia, haemoconcentration, coagulation disorder, oliguria, shock |
Table 1: Golan classification of ovarian hyperstimulation syndrome
The imaging findings of OHSS are similar on ultrasound (US), computed tomography (CT), and magnetic resonance (MR) imaging i.e. bilateral symmetrically enlarged ovaries containing multiple variable-sized cystic lesions representing enlarged follicles or corpus luteum cysts, in the presence of ascites (Figure 1).The distribution of the ovarian cysts may be such as to create a spoke-wheel appearance with thin radiating septa between the cysts and a central hub of ovarian tissue (Figure 2). Haemorrhage may also occur into the cyst (Figure 3) that may result in accentuation of the pain. Similar imaging findings are seen on CT (Figure 4) and MR imaging (Figure 5).
Enlarged hyperstimulated ovaries are also at risk for torsion. The risk is further increased in the presence of ascites and pregnancy. Clinical symptoms are often nonspecific, and ovarian torsion should be suspected and excluded in any female patient undergoing infertility treatment who presents with severe abdominal pain. The most consistent imaging finding is asymmetric enlargement of the torted ovary (Figure 6). The presence of arterial and venous flow on colour Doppler US does not exclude the presence of torsion. Visualisation of the torted ovarian pedicle as the “whirlpool sign” is helpful in making the diagnosis (Figure 7). As with US, the most common finding of ovarian torsion in CT and MR imaging is unilateral ovarian enlargement (Figure 8). Prompt diagnosis of ovarian torsion is essential to prevent irreversible ischemia and infarction. Ovarian salvage is particularly important in patients who are already pregnant and in those desiring future conception.
An ectopic pregnancy is defined as an abnormally implanted embryo. In this case, the blood supply is derived from this abnormal implantation site. As the pregnancy progresses, the potential for rupture is created which could result in massive hemorrhage and death. There is also an increased risk for ectopic pregnancy following ART with a reported incidence in different studies ranging from 2.1% to 8.6%. 82% of ectopic pregnancies are tubal in location; however there is a relative increased risk for rarer and more lethal forms including interstitial and cervical ectopic pregnancies.
Patients with suspected ectopic pregnancy are initially evaluated with quantitative measurement of serum β-hCG in addition to transvaginal US. In general, transvaginal US should demonstrate at least a gestational sac when serum β-hCG levels exceed 2000 mIU/ml. Absence of an intrauterine gestational sac with β-hCG levels above this threshold should raise the suspicion of ectopic pregnancy and trigger a comprehensive search. Failure of the β-hCG level to increase (doubling time of 49 hours) should also raise the suspicion of an ectopic pregnancy. Importantly, 35% of ectopic gestations do not demonstrate an extrauterine mass.
The most common finding in a tubal pregnancy is an adnexal mass separate from the ovary (Figure 9), with increased specificity when it moves independently from the ovary or contains a yolk sac or living embryo with demonstrable cardiac activity. The second most common sign of a tubal pregnancy is the tubal ring sign (Figure 10) that consists of a gestational sac surrounded by a hyperechoic ring. Similar findings may be detected by MR imaging (Figure 11), while residues of blood products in the surrounding structure may indicate ongoing rupture.
Interstitial pregnancy refers to an implanted gestational sac in the intramyometrial portion of the fallopian tube. Symptoms of such an ectopic pregnancy tend to manifest later and rupture may result in catastrophic hemorrhage due to proximity to the uterine artery. At US, an eccentrically located gestational sac surrounded by a thin layer of myometrium measuring less than 5mm may be seen (Figure 12). Cervical ectopic pregnancy is 10 times more common in ART patients and results from embryo implantation in the endocervical canal. US findings include an hourglass-shaped uterus secondary to cervical expansion (Figure 13).
US diagnosis of ectopic pregnancy is particularly challenging in women undergoing fertility treatment as there is a large degree of overlap in the signs and symptoms. Pelvic pain is common following ART, especially in OHSS. Stimulated ovaries are enlarged, which may obscure an ectopic pregnancy. Ascites is often present following ART, especially in the setting of OHSS, and hemorrhagic ascites may result from rupture of a corpus luteum cyst (rather than a rupturing ectopic gestation).
Heterotopic pregnancy refers to simultaneous intrauterine and ectopic pregnancies and has an incidence of 1–3% in ART patients. In women undergoing infertility treatment, careful evaluation of the adnexa is crucial even if an intrauterine pregnancy is documented.
Ultrasonography is the first-line imaging modality for the evaluation of complications of ART, although nonspecific symptoms may sometimes lead to other cross-sectional imaging being performed. Familiarity with the multimodality imaging appearance of these entities will allow accurate and timely diagnosis and help avert potentially fatal consequences.
Figure Legends

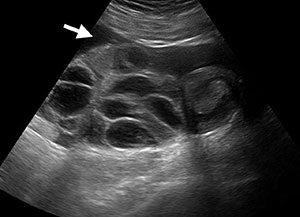
Figure 1: Transvaginal US images of the right (a) and left (b) ovaries in a case of hyperstimulation that presents with ovarian enlargement, numerous large cysts and ascites (arrow in b).

Figure 2: US showing the spoke wheel appearance of ovarian hyperstimulation.
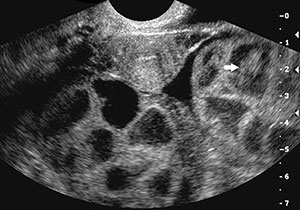
Figure 3: US showing haemorrhage (white arrow) into a cyst in ovarian hyperstimulation. Ascites (black arrow) is also present.

Figure 4: Coronal CT scan in a patient with OHSS shows bilateral ovarian enlargement by multiple cysts (arrows) and mild perihepatic ascites (arrowhead). Uterus (UT).
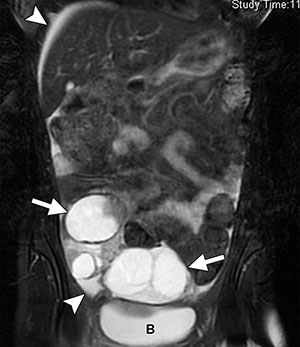
Figure 5: MR image carried out in a patient with OHSS due to clinical suspicion of appendicitis. Coronal fat-saturated T2-weighted image shows bilateral ovarian enlargement (arrows) and mild ascites (arrowhead). Bladder (B).

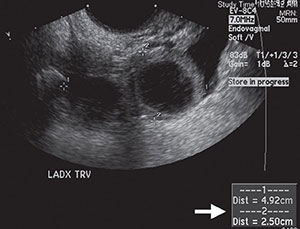
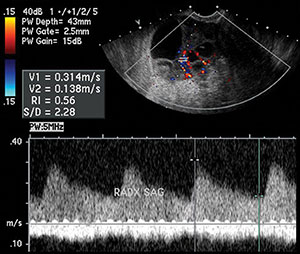
Figure 6: US images show enlarged, multicystic right (a) and left (b) ovaries consistent with OHSS. The right ovary is asymmetrically enlarged (arrow), the only clue to ovarian torsion in this case. (c) Duplex Doppler US image of the right ovary shows arterial and venous flow.

Figure 7: The “whirlpool sign” on colour Doppler US represents the torted ovarian pedicle. Notice the corkscrew appearance of the vessels.
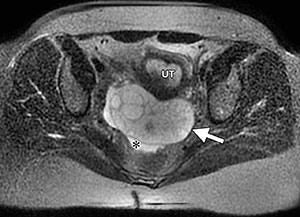
Figure 8: MR scan shows the enlarged torted left ovary (arrow) compared to the right (not seen). Also notice that the enlarged ovary tends to occupy a midline location and no longer lies along the pelvic sidewall. Ascites (*).
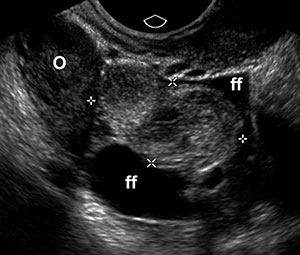
Figure 9: Endovaginal US image shows a paraovarian ectopic pregnancy as a mass (between crosshairs) adjacent to the right ovary (o) with surrounding free fluid (ff).

Figure 10: Endovaginal US image showing the tubal ring sign (arrow) confirming a tubal ectopic pregnancy adjacent to the normal left ovary (arrowheads).
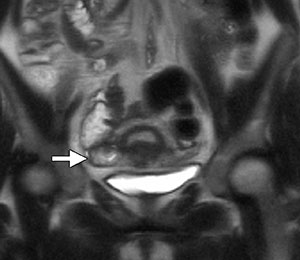
Figure 11: Coronal T2-weighted MRI image shows a tubal ring to the right of the uterus confirming a tubal pregnancy.
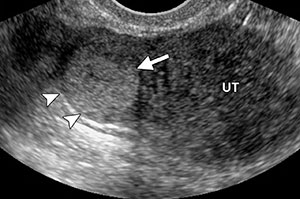
Figure 12: Endovaginal US showing a hyperechoic (haemorrhagic) gestational sac (arrow) eccentrically located in the uterine fundus with a posterior thin myometrial layer (arrowheads).
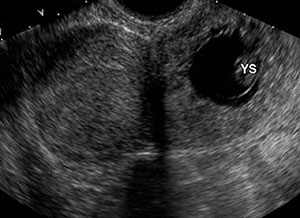
Figure 13: Cervical ectopic pregnancy with a figure eight configuration of the uterus and cervix. A gestational sac containing a yolk sac (YS) is seen in the cervix.