Stroke affecting the eye requires immediate treatment, can signal future vascular events
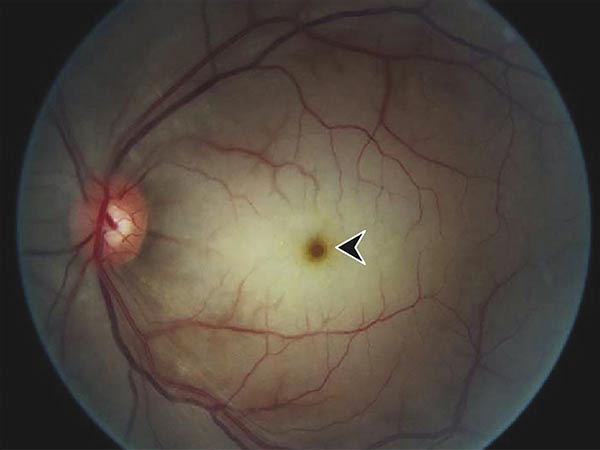
While most people think of strokes affecting the brain, they can also affect the eye. Central retinal artery occlusion (CRAO) is a rare form of acute ischemic stroke that occurs when blood flow is blocked to the main artery of the eye. It typically causes painless, immediate vision loss in the impacted eye, with fewer than 20% of people regaining functional vision in that eye.
The American Heart Association published a new scientific statement, “Management of Central Retinal Artery Occlusion,” in Stroke, an American Heart Association journal. The American Association of Neurological Surgeons/Congress of Neurological Surgeons Cerebrovascular Section affirms the educational benefit of the scientific statement, and it has been endorsed by the North American Neuro-Ophthalmology Society, the American Academy of Ophthalmology Quality of Care Secretariat and the American Academy of Optometry.
“Central retinal artery occlusion is a cardiovascular problem disguised as an eye problem. It is less common than stroke affecting the brain but is a critical sign of ill health and requires immediate medical attention,” said Chair of the statement writing committee Brian C. Mac Grory, M.B.B.Ch., B.A.O., M.R.C.P., an assistant professor of neurology and staff neurologist at the Duke Comprehensive Stroke Center at Duke University School of Medicine in Durham, North Carolina. “Unfortunately, a CRAO is a warning sign of other vascular issues, so ongoing follow-up is critical to prevent a future stroke or heart attack.”
In a comprehensive review of the world literature, committee members from the specialties of neurology, ophthalmology, cardiology, interventional neuroradiology, neurosurgery and vitreoretinal surgery summarized the state of the science in this condition. They found indications that this type of stroke can be caused by problems with carotid arteries, the blood vessels in the neck. However, there is also evidence CRAOs could be caused by problems with the heart, such as atrial fibrillation. The risk of having a CRAO increases with age and in the presence of cardiovascular risk factors such as hypertension, hyperlipidemia, Type 2 diabetes, smoking and obesity.
The new scientific statement notes the lack of large clinical trials on CRAOs leads to uncertainty within the medical community of exactly what causes them or the best way to treat them. As a result, there is wide variability in diagnosis and treatment methods. Most concerning, according to Mac Grory, is that many practitioners may not recognize CRAO as a form of stroke resulting in patients receiving delayed testing and treatment, often in the outpatient clinic instead of the emergency department.
“We know acute CRAO is a medical emergency requiring early recognition and triage to emergency medical treatment,” Mac Grory said. “There is a narrow time window for effective treatment of CRAO and a high rate of serious related illness. So, if a person is diagnosed in a doctor’s office or other outpatient clinic, they should be immediately sent to a hospital emergency department for further evaluation and treatment.”
Current literature suggests that treatment with intravenous tissue plasminogen activator (tPA), a “clot buster” that is also used to treat brain strokes, may be effective. But tPA must be administered within 4.5 hours of the first sign of symptoms to be most effective and safe.
The writing committee also noted that emerging treatments, such as hyperbaric oxygen and intra-arterial alteplase, show promise but require further study. Other potential treatments that require further research and evaluation include novel thrombolytics to break up clots and novel neuroprotectants for use in tandem with other therapies to restore blood flow in the blocked artery.
Because of the potential for future strokes or even heart attacks, patients should undergo urgent screening and treatment of vascular risk factors. The writing committee notes that the complexities of diagnosing and treating CRAOs require a team of specialists working together. Secondary prevention (including monitoring for complications) must be a collaborative effort between neurologists, ophthalmologists, cardiologists and primary care clinicians. Risk factor modification includes lifestyle and pharmacological interventions.
Source: American Heart Association
Full bibliographic information
Management of Central Retinal Artery Occlusion A Scientific Statement From the American Heart Association
Stroke. 2021;52:00–00.