
The role of NSAIDs in colorectal cancer prevention: a literature review
Abstract
Inflammation has long been associated with cancer. COX enzymes play an integral role in inflammation. NSAIDs act on COX enzymes to reduce inflammation. The efficacy of NSAIDs was considered in cancer prevention and on survival thereafter. Aspirin was found to be the most superior NSAID but it also prolonged the survival of cancer patients and provided anti-thrombotic protection.
Introduction and Methodology
CRC has been on the rise since the 1970s and in 2012, there were 225 new cases, mostly in the 65 to 69 age bracket (no sex difference in occurrence). The highest incidence per 100,000; in females occurred in the 80-84 age group whilst in males it occurred in those aged over 85, with the incidence rate being that of 275.18 and 401.79 respectively (1).
NSAIDs are drugs which reduce inflammation by inhibiting COX-1 and COX-2, but also interact with DNA mismatch repair genes, inhibit lipid mediators (such as sphingosine-1-posphate) and induce NAG. The pathway of NSAIDs is common but some will inhibit one part of the pathway (the prostaglandin forming pathway) more than others. The commonest types of NSAIDs are; Aspirin, Ibuprofen and Diclofenac.
This literature review analysed studies relating the effect of NSAIDs to CRC and articles between the year 2000 and 2015 were considered.
Mechanism of Action of NSAIDs
NSAIDs are drugs which act as reversible non-selective inhibitors of COX. COX is responsible for the conversion of arachidonic acid to prostaglandins (PGF2 α, PGI2, PGD2 and PGE2) and thromboxane A2. COX is composed of 2 enzymes; COX 1 (expressed in most tissues and described as the “housekeeping” enzyme, regulating normal cellular processes) and COX 2 (usually undetectable whose expression is increased during inflammation). NSAIDs also influence and inhibit lipoxygenase formation from arachidonic acid to leukotrienes (2). Figure 1 shows both mechanisms of action of NSAIDs.
Aspirin blocks COX-1 and COX-2 and induces the synthesis of lipoxins and resolvins (lipid mediators with anti-inflammatory properties) that can be made from arachidonic acid and EPA. Side effects of aspirin include stomach ulcers and impaired blood clotting. Aspirin also acts upon the Bcl family proteins (regulate mitochondria dependent apoptosis) by reducing their concentrations and inducing apoptosis in a large number of cancer cells (3). Ibuprofen is a non-selective inhibitor of COX, however its pharmacological effects are due to its inhibition of COX-2. Ibuprofen reduces inflammation, pain, swelling and fever by inhibiting prostaglandin synthesis (4).
Inflammation and Cancer
A cancer is a neoplastic change to a tissue. Many types of cancers arise from sites of infection, chronic irritation and/or inflammation. Irritation in itself leads to micro inflammation and then onto chronic diseases (Crohn’s disease, chronic reflux oesophagitis and Barrett’s oesophagus); with cancer being one of them (15-20% of cancer deaths can be linked to inflammation and infections (5). Inflammation can become chronic leading to a change in the microenvironment of cells, disrupting cancer-related genes and cell signalling proteins which are involved in DNA repair, the cell cycle and apoptosis. This results in an increased number of unresolved cell mutations leading to neoplastic changes. It is logical to assume that anti-inflammatory interventions will help to limit cancer development and progression.
COX is a major enzyme in the inflammatory pathway. NSAIDs may be used to block it and inhibit inflammation in the acute and chronic stage. In many types of cancers, COX-2 is inadequately regulated and prostaglandin E synthase expression is abolished, resulting in an increased concentration of prostaglandin E2. Overexpression of prostaglandin E2 can be seen in early stage colon cancer (6).
Tumours are not solely made up from cancer cells but from other cells which make up the stroma such as; fibroblasts and leukocytes. Cancer cells can undergo rapid proliferation and the site becomes necrotic and hypoxic due to the high demands of these cells. To compensate, tumour cells send out growth factors and cytokines (colony stimulating factor-1 and transforming growth factor – beta) to attract monocytes and macrophages. This leads to more cells being recruited, which will exacerbate the inflammation process (5).
 and COX (leading to prostaglandin formation)")
")
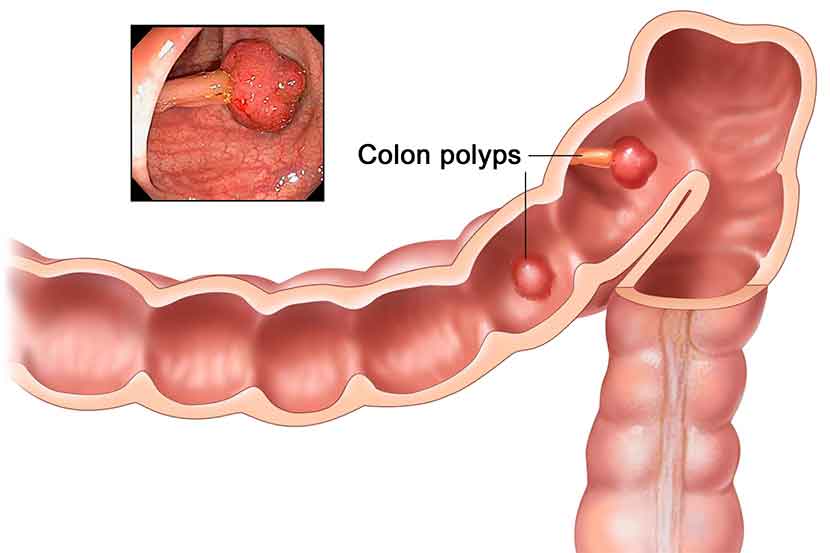
Colorectal cancer pathogenesis and genes involved
CRC is initiated by; CIN, CIMP or MSI. The CIN pathway is the commonest type and is due to accumulation of chromosomal abnormalities (structural and numerical) resulting in aneuploidy (8). The second commonest pathway is the CIMP pathway, which provides epigenetic instability for spontaneous cancers to methylate the promoter regions which results in inactivation of TSGs such as MLH1 (9). Numerous nucleotide repeat sequences (known as microsatellites) exist scattered throughout the human genome. DNA polymerase is prone to errors when copying these sequences, but MMR function usually repairs them. In cases where MMR is not functioning well, MSI will occur (10).
Inflammation is involved in both sporadic and heritable colon cancer cases. CRC can be either due to sporadic mutations or colitis-associated colon cancer. CRC occurs due to mutations to oncogenes and/or tumour suppressor genes (TSG). The APC tumour suppressor gene and its gene product, APC, play a role in the maintenance of colonic epithelium. The APC gene can be inactivated, resulting in decreased APC protein product. Since APC modulates COX-2 expression, a mutant APC protein product results in over-expression of COX-2 (12).

The KRAS has a role in the CIN and CIMP pathways. The protein product of the KRAS gene is important in normal tissue signalling and a mutation can cause a loss of GTPase activity and hence constitutive signalling. (13).
TP53 is a gene whose product p53 regulates the cell cycle. p53 usually slows the cell cycle to repair any DNA damage. Mutations on chromosome 17 can result in a mutation in the TP53 gene, resulting in impaired p53 production. Impaired p53 is unable to arrest the cell cycle resulting in damaged DNA and ultimately tumour formation.
Role of NSAIDs on colorectal cancer gene expression
NSAIDs work primarily on COX-2 (14). This was highlighted by patient’s better response to NSAIDs when they had an elevated COX-2 expression when compared to those with low COX-2 levels. Patients with APC deficiency had elevated COX-2 expression and more aggressive tumourigenesis (15). Inhibition of COX-2 seems to be the key to prevent CRC. 75-100mg of aspirin daily completely blocks COX-1. When aspirin was given at higher doses (325 or 650mg), there was a 50-70% decrease in prostaglandin production and an improved outcome. Apart from exhibiting COX-1 activity, a unique feature of aspirin is the fact that it is the only NSAID which acetylates COX-2, which causes COX-2 to start producing LXA4 instead of PGE2 resulting in an anti-inflammatory effect and inhibition of proliferation of tumour cells (16).
FAP is a condition in which benign polyps form in the colon and rectum, which, if left untreated turn to malignant cells. Investigation of the effects of celecoxib was done by (17) and found that large doses are effective but there are increased deaths from cardiovascular events and hence its use is limited. It concluded that, aspirin is still the NSAID of choice for prevention of CRC arising from FAP.
Prevention of CRC is not always possible hence NSAIDs may be given to lengthen the five year survival period. Study (18) concluded that NSAIDs (most notably aspirin) were associated with a substantial increase in overall survival. They noted that patients who were started on aspirin after they were diagnosed with CRC had a better outcome and longer survival. Other NSAIDs (ibuprofen and diclofenac) did not improve survival rates. They suggested that daily use of low dose aspirin is cost effective and a much better alternative for chemotherapy or radiotherapy, especially in elderly frail patients (18).
Ibuprofen was marketed in 1984 and CRC incidence fell from 57 per 100,000 persons in 1985 to 49 per 100,000 in 2002 (20). During their study they have shown that around 10% of all elderly patients are on some kind of NSAID daily and CRC risk amongst these patients is the lowest when compared to the other 90% of the elderly population. However, due to the side effects of NSAIDs (mainly gastrointestinal (GI) bleeding) they suggested that NSAIDs should only be given to patients who are at a high risk for developing CRC. High risk patients include those with a familial history of CRC and chronic inflammatory diseases.
Conclusion
COX-2 inhibitors are the ideal treatment for CRC, but the only selective COX-2 inhibitor was celoxib (which carries significant side effects). (20) suggested that ibuprofen was also effective but should only be given to patients with a high risk of developing CRC.
These studies have shown that aspirin was the preferred NSAID in CRC prevention (17-19). They also remarked that aspirin increases the risk of CRC prevention and increases the survival rate after CRC was diagnosed. Moreover, low dose aspirin provided moderate chemo preventative effect on adenomas in the large bowel (20).


{kind=link}
{kind=link}