
Ultrasound of the Inguinal Canal – Part I
Pierre Vassallo
Ultrasound has a major role in detecting disease in the inguinal region. A good knowledge of the anatomy and pathologic findings on ultrasound is required to reach a correct diagnosis.
The structure and function of the inguinal canal can only be appreciated when one understands what occurs at this site during the embryonic and fetal periods. The formation of the inguinal canal starts at the 7th week of gestation. In males, it represents the passage through which the testis passes from its intraabdominal location of origin to the scrotum, its normal location at birth. In females, it contains the round ligament of the uterus.
At around 7 weeks of gestation, the gonads (testes and ovaries) develop along with the kidneys from the urogenital ridges. The urogenital ridges are located on either side of the structures that will form the lumbar spine. The more medially located portion of the urogenital ridge forms the gonad and the lateral portion forms the kidney (Fig 1). A ligament called the gubernaculum is attached to the inferior pole of the gonad and extends inferiorly through the abdominal wall into the inguinal region to attach to the labroscrotal fold; the labroscrotal fold forms the scrotum in males and the labia major in females. In female fetuses, the gubernaculum is attached to the uterus in its mid-section. In male fetuses, the gubernaculum shortens and pulls the testis down from its original position near the spine into the scrotum (Fig 2). Due to the attachment of the gubernaculum to the uterus in female fetuses, the migration of the ovary halts near the uterus and the distal gubernaculum forms the round ligament.
All layers of the abdominal wall extend along the gubernaculum, testis and round ligament; they form the scrotal sac in the male (Fig 2). The passage through the different abdominal wall layers represents the inguinal canal, which contains the spermatic cord in the male and the round ligament in the female. An invagination of peritoneum that follows the testis into the scrotum, detaches from the main peritoneal cavity and forms the tunica vaginalis. This peritoneal invagination closes in the female. A persistent peritoneal communication in the male is called a patent processus vaginalis (Fig 3), while in the female, it is called the canal of Nuck. A persistent processus vaginalis predisposes to an indirect inguinal hernia and a communicating hydrocoele.
The inguinal canal is circa 4cm long and extends above the inguinal ligament through the layers of the abdominal wall muscles, starting internally at the internal inguinal ring that lies just lateral to the origin of the inferior epigastric vessels and ending externally above and medial to the pubic tubercle (Fig 4). On ultrasound, the inguinal canal can be traced along its path, starting at the internal inguinal ring and extending to the external inguinal ring (Fig 5).
Inguinal hernias
An indirect inguinal hernia results from the passage of intraabdominal contents into the inguinal canal through the internal inguinal ring. Whereas a direct inguinal hernia passes directly through the abdominal wall layers and does not follow the inguinal canal. An indirect inguinal hernia therefore passes lateral to the inferior epigastric vessels while a direct inguinal hernia courses medial to them (Fig. 6).
Direct and indirect inguinal hernias are usually more evident when the patient increases his/her intraabdominal pressure (e.g. during Valsalva manoeuvre or in the standing position). Consequently, dynamic ultrasound examination at rest, during Valsalva and in the standing position are necessary to detect an inguinal hernia since a hernia may be fully reduced at rest. In addition, dynamic examination will help distinguish reducible from incarcerated hernias, since the latter do not reduce even on compression with the probe (Fig 7). Thickening of the contents of the hernial sac and associated fluid collections are signs of strangulation of the hernia contents (Fig 8). Strangulation may also be noted through the absence of blood flow on colour Doppler ultrasound examination.
The more common complications of surgical hernia repair include seromas, haematomas and abscesses at the site of repair. These are readily detected by ultrasound (Fig 9). Abscesses tend to appear in the late post-operative period (usually after 30 days) and are accompanied by clinical signs of infection. A further post-operative complication of hernia is repair is hernia recurrence, which is also readily detected by ultrasound.
Figure Legends
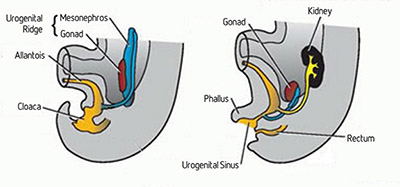
Figure 1. The kidney and gonad develop from a common structure, the urogenital ridge, that is located next to the structures that will form the lower spine in the embryo. The inner part of the urogenital ridge forms the gonad that descends into the pelvic/scrotal area, while the lateral part forms the kidney that retains its paraspinal location.
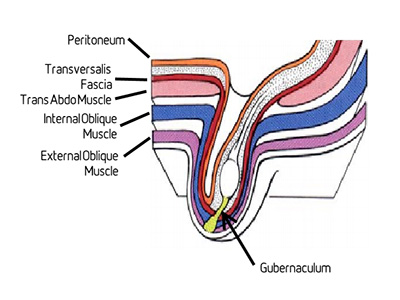
Figure 2. The gubernaculum is attached to the inferior pole of the gonad proximally and into the labroscrotal fold inferiorly. It shortens from the 7th week of gestation onwards and pulls the gonad inferiorly. In males, the testis descends into the scrotum. Due to the attachment of the gubernaculum to the uterus in females, the ovary halts next to the uterus and the distal gubernaculum forms the round ligament. All abdominal wall layers extend along the gubernaculum and around the testis to form the scrotum in males. The path through which the testis and round ligament pass represents the inguinal canal.
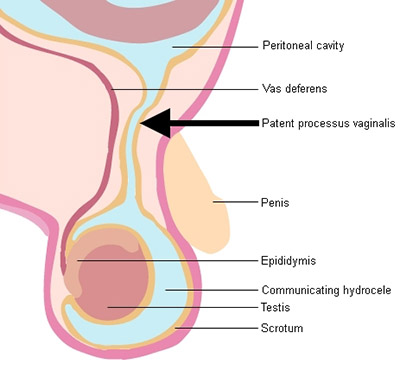
Figure 3. Diagram showing a patent processus vaginalis (arrow) communicating the peritoneal cavity with the tunica vaginalis; this is called a communicating hydrocoele.
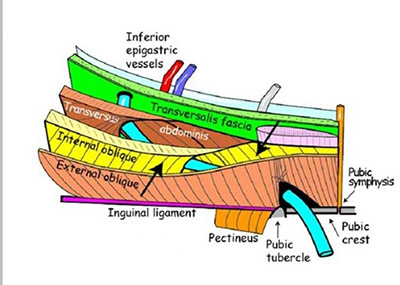
Figure 4. Anatomy of the inguinal canal (arrows). The anterior wall is formed by the external and internal oblique muscle aponeuroses and the posterior wall is composed of the transversus abdominis aponeurosis and the conjoint tendon; the latter is formed by fusion of the distal rectus abdominis tendon with the proximal adductor longus tendon.
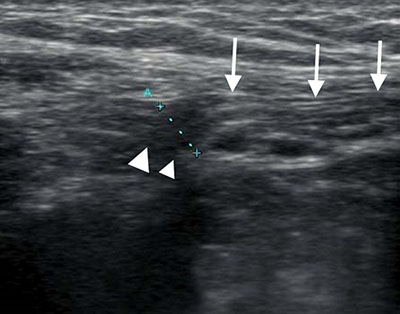
Figure 5. Ultrasound scan parallel to the course of the inguinal canal, showing the internal inguinal ring (arrowheads) and the inguinal canal (arrows) with its contents.
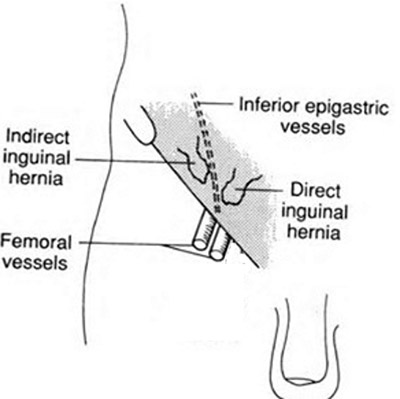
Figure 6. A direct inguinal hernia passes lateral to the inferior epigastric vessels, while a direct inguinal hernia courses medial to them.
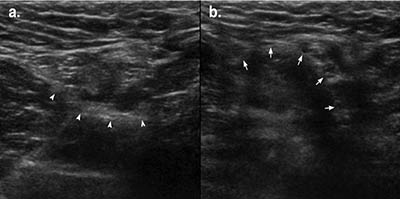
Figure 7. Ultrasound scan of an indirect inguinal hernia showing the inguinal canal at rest (a) and during Valsalva maneouvre (b): note the expansion of the inguinal canal that occurs with increased intraabdominal pressure (arrows).
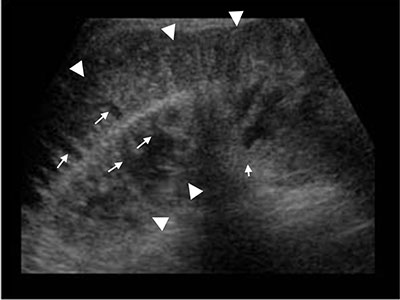
Figure 8. Ultrasound scan showing a thickened loop of small bowel (arrowheads) in the inguinal canal that did not alter with Valsalva manoeuvre and did not reduce on compression. Also note the thickened mucosal folds (arrows); the thickened bowel wall and bowel loops are indicative of hernia strangulation.
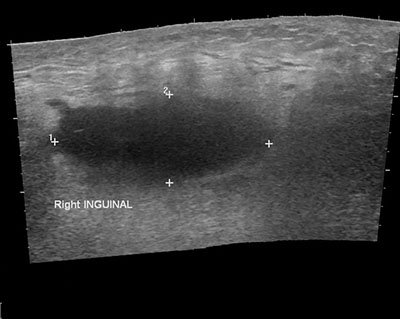
Figure 9. Ultrasound scan showing a fluid collection (calipers) at the site of a hernia repair in the early post-operative period.
