Breast cancer imaging: ductal carcinoma in-situ (DCIS) – Part I
Pierre Vassallo
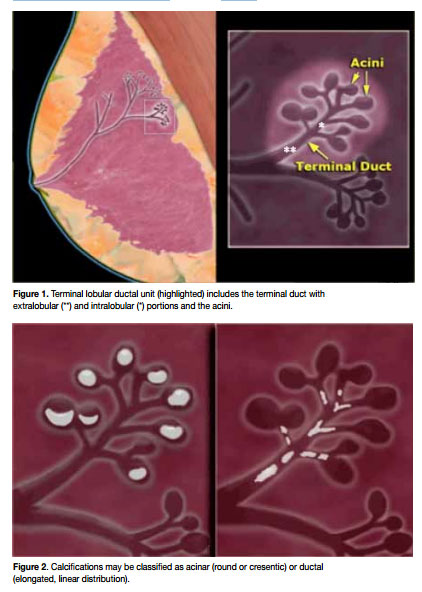
Ductal carcinoma in-situ (DCIS) is a noninvasive malignancy and a potential precursor to invasive cancer at pathologic analysis, DCIS shows proliferation of malignant epithelial cells that line the ducts (at the level of the terminal ductal–lobular unit) (Fig 1) without invasion through the basement membrane The detection rate of DCIS has increased markedly over the past two decades with the advent of breast cancer screening. Early detection and assessment of extent of DCIS is important for planning successful conservative breast surgery. Half the cases of recurrent DCIS are associated with invasive ductal cancer. In addition, 20% of patients with DCIS develop metastases within 10 years of initial diagnosis.
In the following article, we will review the findings of DCIS on mammography and breast ultrasound (US) and also discuss the role of breast Magnetic Resonance Imaging (MRI) for improved detection of DCIS.
Over 90% of cases of DCIS are detected as microcalcifications on mammography. These calcifications are calcified cellular debris or secretions within the intraductal lumen. The uneven calcification of the cellular debris explains the fragmentation and irregular contours of the calcifications.
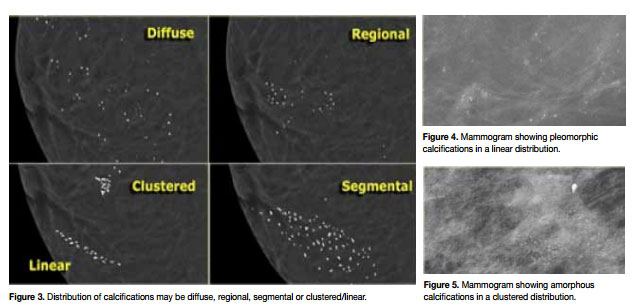
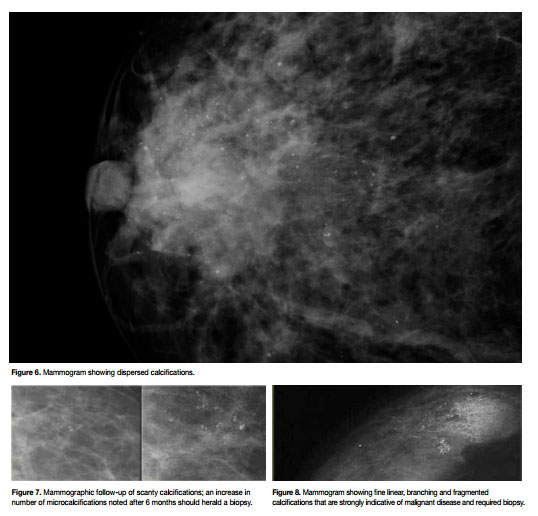
Figure 2 shows the distinction between linear and rounded microcalcifications that helps distiguish acinar (mostly benign) from ductal (suspicious for malignancy)- type calcifications. Calcifications are extremely variable in size, density and form; they may be amorphous (morphus means form in Greek, amorphus means no particular form), pleomorphic (pleo is Greek for more or many forms), heterogeneous (mixed density), rounded, coarse (≥5mm) or fine (<5mm). Their distribution may be clustered, linear, or segmental (Fig 3). The diagnostic approach to breast calcifications is to analyze the morphology, distribution and sometimes change over time. Pleomorphic calcifications distributed in a linear fashion or in a cluster (>5 calcifications in an area of 1cm diameter) should raise enough suspicion to advise biopsy (Fig 4). The presence of amorphous (Fig 5) or rounded calcifications in a linear or clustered distribution may also lead to biopsy, however the level of suspicion is lower in these instances. Dispersed or regional distribution of calcifications in one or both breasts or in multiple foci is usually indicative of benign disease (Fig 6). A segmental distribution of calcifications especially in the absence of pleomorphism is of indeterminate significance; in such situations or when calcifications are scanty in number, a close mammographic follow-up may be justified (Fig 7). Fine linear and branching calcifications, particularly when fragmented, require biopsy (Fig 8).