
Childhood Mortality in Malta – how do we fair?
Kathleen England
Introduction
Mortality among children of all ages has fallen markedly over the past 30 years. Reduction in childhood mortality remains high on the international agenda as witnessed by the millennium development goal 4 (MGD 4),1 which aimed at reducing the mortality rate of children under five years of age by two thirds between 1990 and 2015. Though global under-five mortality has been reduced by more than a half, the goal of reducing it by two-thirds has not been reached. Timely, local and valid assessments of trends in child mortality along with the associated drivers of these trends can provide an important input to national, regional, and global debates on the next steps which need to be undertaken.2
According to the European Observatory on Health Systems and Policies,3 amongst all EU countries, Sweden was the country with the lowest mortality rate in children 0-14 years of age with a rate of 29.27 per 100,000. Romania and Bulgaria had the highest mortality rate, with rates reaching 116.8 per 100,000 in Romania. Malta placed 19th out of the 27 participating countries with a reported rate of 56.16/100,000 population. However, one must keep in mind that Malta is the only European country where termination of pregnancy is completely illegal. Mortality in the 0-14 year olds is mainly due to deaths occurring in the 1st year of life (infant mortality). In view of this fact, having no termination of pregnancy means that infants who may be aborted in other countries due to congenital anomalies which may be fatal, would be born alive and often die in the first year of life in Malta. This contributes to increased childhood mortality. This has been well documented in a study by Gatt M et al4 which showed that, in comparison to other member states, the higher reported neonatal mortality rates in Malta are mainly attributed to lethal congenital anomalies.
Throughout the early years of life, post-infancy may still be influenced by conditions present at birth. However, many lethal congenital anomalies would have resulted in death during the first year of life and therefore, the effect of congenital anomalies on deaths beyond one year is reduced. The aim of this study was to assess trends in childhood mortality for Malta beyond one year of age and compare rates with that of other European countries.
Methodology
Using Mortality data for Malta from the WHO Mortality Database as well as the National Mortality Registry at the Directorate for Health Information and Research, mortality data for infants aged 0-1 year and those aged 1-14 years of age was extracted from 1980-2012. Similar population figures were extracted and age-specific mortality rates from 1980-2012 were calculated. These trends and rates were compared to rates from a number of countries for which data was similarly extracted from the WHO database. The countries used for this analysis were Sweden, which according to Wolfe et al5 ranks lowest in childhood mortality, Greece representing a southern European country, United Kingdom representing a country from EU-15, Ireland and Poland which have similar laws regarding abortion and Slovenia which is a new accession country. In addition, an average mortality rate over 5 years for children aged 1-4 years, 5-9 years and 10-14 years was calculated for Malta and compared to the average for the European Union.
Trends in causes of death for children 1-14 years of age for EU-15, as depicted by Wolfe et al,5 were then compared to those for Malta, in order to assess whether a similar pattern in the shift in causes of death is happening in Malta and the EU-15.
Results
Trends in childhood mortality rates in Malta compared to EU countries
Mortality rates in 0-14 years of age have been showing a decreasing trend in all countries presented, as seen in Figure 1. Deaths in this age group are principally attributed to infant mortality. Due to small numbers for Malta, a 3-year moving average has been used. Moving average is a calculation to analyze data points by creating a series of averages in order to smooth out short-term fluctuations useful especially with data involving small numbers. Whilst Malta’s mortality rates in this age group are amongst the highest, this decreases in the 1-14 year age group (Figure 2), where Malta’s rates overlap with most countries.
Figure 1. Age-specific mortality rates 0-14 years per 100,000 population
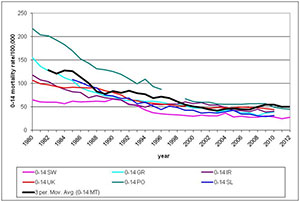
SW-Sweden; GR-Greece; IR-Ireland; UK-United Kingdom; PO-Poland (missing data 1997-1998) ; SL-Slovenia; MT-Malta (3 year moving average)
Figure 2. Age-specific mortality rates for 1-14 years per 100,000 population
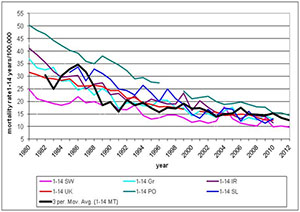
SW-Sweden; GR-Greece; IR-Ireland; UK-United Kingdom; PO-Poland (missing data 1997-1998); SL- Slovenia; MT-Malta (3 year moving average)
If one compares age specific childhood mortality in Malta to the EU average, in the age groups between 1-14 years, where the effect of congenital anomalies is decreased Malta’s rates are much closer to the EU average (Table 1).
Table 1: Age-specific mortality rates per 100,000 population in Malta compared to the EU 28 average
| Age of child |
Malta (5 year average 2008-2012) |
EU average for 2011 |
| 0-1 | 627.6 (lower CI 525.9;upper CI 748.3) | 392.8 |
| 1-4 | 23.8 (lower CI 14.8; upper CI 38.0) | 18.4 |
| 5-9 | 6.0 (lower CI 2.4; upper CI 13.7) | 9.7 |
| 10-14 | 13.6 (lower CI 8.0; upper CI 22.5) | 11.1 |
Shift in Causes of Death in 1-14 year olds in Malta and EU-15
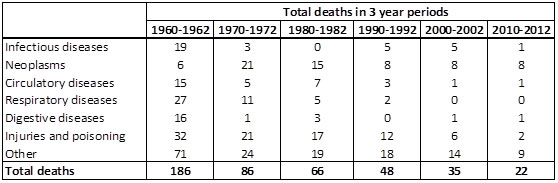
A shift in the main causes of childhood mortality in 1-14 year olds has taken place over the years as seen in figures 3 and 4 and table 2, with mortality due to infectious diseases, respiratory diseases and gastrointestinal diseases decreasing, while deaths due to neoplasms becoming more predominant. ‘Other’ causes of death mainly include congenital anomalies, endocrine and neurological disorders. While trends are similar in EU-15 compared to Malta for most causes, injuries are a less frequent cause of death in 1-14 year olds in Malta compared to EU-15, while neoplasms are a more frequent cause of death locally. However, numbers for Malta are very small and need to be interpreted cautiously (Table 2).
Figure 3. Shifting relative cause mortality in children 1-14 years in the 15 pre-2004 countries of the EU, 1960-20105
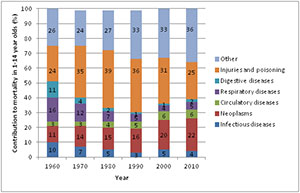
Figure 4. Shifting relative cause mortality in children 1-14 years in Malta, 1960-2012
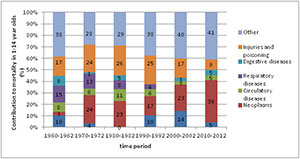
Table 2. Main causes of death in Malta in different time periods in 1-14 year olds
Discussion and some Conclusions
Infant and childhood mortality represent an important indicator of the health care system of a country. Mortality rates after one year of age in Malta are much closer to the EU average, compared to those under one year of age. In Malta, while childhood neoplasms are increasingly contributing to a larger percentage of deaths (3.2% in 1962 vs 36.4% in 2012), both the overall number of deaths as well as deaths from neoplasms are decreasing.
Non-communicable diseases are increasingly becoming common causes of childhood illness and death. Health services and social and cultural determinants (conditions in which people are born, grow, work, live, and age) contribute to differences in health outcomes. Development of systems more responsive to evolving child health needs is likely to necessitate reconfiguring of health services as part of a whole-systems approach to the improvement of health.5
References
1. United Nations. Millennium Development goals and beyond 2015. Accessed 4th February 2015. Available from: www.un.org/millenniumgoals/news.shtml
2. Wang H., Liddell C., Coates M. Global, regional, and national levels of neonatal, infant, and under-5 mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014; 384(9947):957–79.
3. Wolfe I, Mckee M. Strengthening child health and health services. European Observatory on Health Systems and Policies. 2014.
4. Gatt M, England K, Grech V, Calleja N. Contribution of Congenital Anomalies to Neonatal Mortality Rates in Malta. Paediatric and Perinatal Mortality Epidemiology. 2015; 29(5):401-6.
5. Wolfe I, Thompson M. Health Services for children in Western Europe. Lancet. 2013; 381:1224-34.