
Hypertonic saline nasal irrigation in the management of allergic rhinitis and chronic sinusitis
by David Grech
Allergic rhinitis is a disease characterized by the classic symptoms of rhinorrhea, obstruction of the nasal passage, sneezing and itching, all occurring in a temporal relationship to allergen exposure.1 Conventional treatment options include antihistamines, decongestants, anticholinergics and corticosteroids. 1,2
If untreated or in the long term, chronic inflammation of the maxillary sinuses may result in increased secretions from the sinuses and postnasal drip caused by the allergic response. The mucosa becomes swollen and hypertrophic. The impaired drainage of the secretion from the sinuses (especially from the maxillary sinuses) increases the likelihood of recurrent infections. The conventional medical approach to chronic sinusitis includes treatment with local and systemic anti-inflammatory drugs with or without antibiotics. 3
Many patients with sinusitis also experience chronic cough, fatigue and lassitude characteristic of the disease. The prevalence of chronic sinusits among patients with respiratory complaints is estimated to be as high as 38% in children older than 10 years of age. 3
Recent studies have documented interesting results using nasal irrigation as an adjunctive treatment modality in many sinonasal diseases. In this regard, it has also been reported that an increased efficacy could be effected using hypertonic (2 – 3.5% w/v) saline instead of normal saline. 4
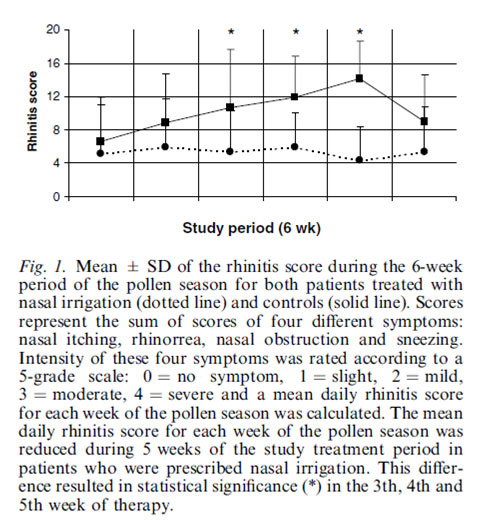
Significant clinical benefits were observed in children with seasonal allergic rhinitis who received a regimen of three-times daily nasal irrigation with hypertonic saline during the pollen season (Figure 1). Indeed, the mean daily rhinitis score was reduced during the study treatment period (6 weeks). Reduced need for oral antihistamines was also observed. 1
Tamooka et al. have also reported that nasal wash is efficient in the treatment of seasonal allergic rhinitis in adults. 5 These authors documented a significant improvement in the symptoms score after nasal irrigation with hypertonic saline.
It has been shown that the hyperosmolar airway fluids resulting from hypertonic saline nasal irrigation (HSNI) increase ciliary beat frequency, possibly by regulating the use or availability of adenosine triphosphate by the ciliary axoneme. This enhances mucociliary clearance, facilitating the evacuation of potentially allergen- and irritant-containing mucus. The topical antibacterial effect of hypertonic saline solution is also well established in wound dressing and washing of open wounds. 4
In summary, daily HSNI is a safe, effective and tolerable therapy associated with high patient satisfaction, improved quality of life, decreased antibiotic use, and improved sinus symptoms in both paediatric and adult patients with a history of frequent rhinosinusitis and chronic sinus complaints. Study participants also expressed satisfaction in their perception that at-home use of HSNI reduced the number of trips to their physician and the number of antibiotic prescriptions. 3
Source : Garavello W et al Hypersaline nasal irrigation in children with symptomatic seasonal allergic rhinitis: A randomized study. Pediatr Allergy Immunol 2003; 14: 140-143
References
- Parikh A, Scadding GK. Seasonal allergic rhinitis. Br Med J 1997; 314: 1392–5.
- Garavello W et al. Hypersaline nasal irrigation in children with symptomatic seasonal allergic rhinitis: A randomized study. Pediatr Allergy Immunol 2003; 14: 140-143
- Rabago D et al. Qualitative aspects of nasal irrigation use by patients with chronic sinus disease in a multimethod study. Ann Fam Med 2006;4: 295-301
- Shoseyov D et al. Treatment with hypertonic saline versus normal saline nasal wash of pediatric chronic sinusitis. J Allergy Clin Immunol 1998; 101: 602-5
- Tomooka LT, Murphy C, Davidson TM. Clinical study and literature review of nasal irrigation. Laryngoscope 2000; 110: 1189–93.

{kind=link}