Inflammatory Breast Cancer
Pierre Vassallo

Inflammatory breast cancer (IBC) is a rare subtype of breast cancer that accounts for 2–5% of all breast cancers. It has a highly virulent course with a low 5-year survival rate of 25–50%. Standard treatment with preoperative chemotherapy, mastectomy, and radiation therapy has been shown to improve prognosis.
IBC usually presents with rapid onset of clinical signs that develop within 3 months which include breast erythema and edema, often with no palpable mass,and may involve one-third or more of the breast (Fig 1). Peau d’orange (french for “orange skin”) may also be present where the skin is pitted and dimpled due to the presence of tumor emboli that obstruct the dermal lymphatics (Fig 2). The breast may be enlarged, warm, and tender. These symptoms may mimic inflammation, however there is no true inflammatory component to IBC. 20–40% of patients will already have distant metastases, which reflects the very aggressive nature of IBC.

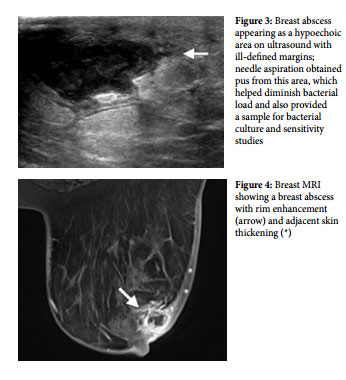
IBC usually presents with rapid onset of clinical signs that develop within 3 months which include breast erythema and edema, often with no palpable mass,and may involve one-third or more of the breast (Fig 1). Peau d’orange (french for “orange skin”) may also be present where the skin is pitted and dimpled due to the presence of tumor emboli that obstruct the dermal lymphatics (Fig 2). The breast may be enlarged, warm, and tender. These symptoms may mimic inflammation, however there is no true inflammatory component to IBC. 20–40% of patients will already have distant metastases, which reflects the very aggressive nature of IBC.or an incomplete response to antibiotic treatment within 1–2 weeks, malignancy such as IBC should be considered. Breast abscess formation presents as a ring enhancing lesion on MRI with adjacent skin thickening (Fig 4).

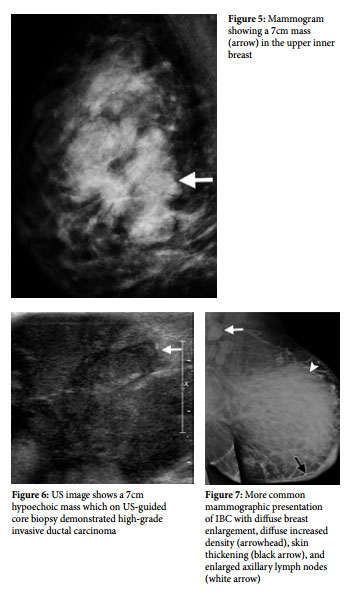
Locally advanced breast cancer (LABC) may also present with a similar clinical picture, however the onset of IBC occurs within a short period (usually 3 months) whereas that of LABC is more protracted. Erythema and skin induration (and peau d’orange) are less common, but may be present if skin infiltration by tumor cells occurs. Mammography of LABC will show a large mass (Fig 5) that may have been present clinically for a long time, while ultrasound shows a solid hypoechoic mass (Fig 6). Attempts at aspiration show no pus or fluid and histologic diagnosis is established by US-guided core biopsy. Skin punch biopsy is utilized to confirm cancerous infiltration of the skin, which is a feature of IBC.
LABC occurs in an older age group and has a better prognosis than IBC since it is less aggressive and grows more slowly. In LABC, the incidence of distant metastases is lower (10% in LABC vs 20-40% in IBC) and its genetic subtypes are more likely to respond to therapy; LABC is more likely to be oestrogen-receptor (ER) positive and less likely to be HER2 negative, while IBC has a high incidence of triple-negative cancers (50%) and is more frequently HER2 positive (40%). Functioning tumor suppressor gene (p53 gene) is lower in IBC and multiple genetic factors that stimulate tumor growth are more likely to be present.
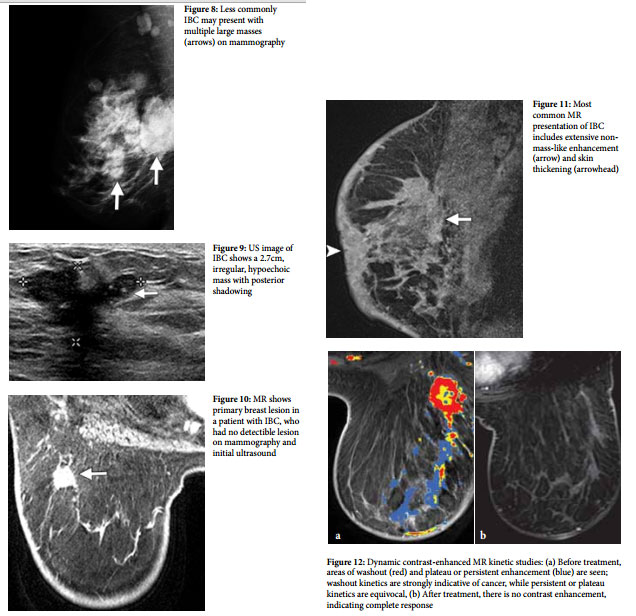
In the imaging workup of IBC, mammography is usually the initial study that shows diffuse enlargement of the breast with diffusely increased density, skin thickening and possibly enlarged lymph nodes (Fig 7). A less common mammographic presentation of IBC is that of multiple masses (Fig 8). US can help differentiate a benign cystic mass from a solid mass and can evaluate a solid mass according to its margins (smooth, irregular, or speculated), its size and extent (Fig 9). If no mass lesion is detected on mammography or US, Magnetic Resonance Imaging (MRI) may be used to target biopsy as it has been shown to be the most accurate imaging technique for detection of the primary breast lesion in patients with IBC (Fig 10). The primary breast lesion is detected at mammography in 68–80% of cases, at US in 94–95% of cases, and at MRI imaging in 98–100% of cases. The more commonappearance of IBC on MRI is however as a diffuse contrast enhancing area involving a large part of the breast, with skin thickening (Fig 11); presentation as a mass-lesion is less common on MRI. Involvement of the pectoralis major muscle and axillary, supraclavicular and internal mammary lymph nodes as well as the contra-lateral breast are common in IBC and are also best assessed with MRI. Evaluation for distant metastatic disease from IBC would require Computed Tomography (CT), MRI or [18F]- fluorodeoxyglucose (FDG) Positron Emission TomographyComputed Tomography (FDG PET/CT).