Intermittent calf-muscle electrical stimulation on walking capacity in patients living with type 2 diabetes mellitus and intermittent claudication
Christian Ellul & Alfred Gatt
| Abstract
A prospective, one-group, pretest-posttest study design was employed on forty participants (n=40) with bilateral limb ischemia (ABPI <0.90), diabetes mellitus and calf muscle claudication. Participants received a fixed program of calf muscle electrical stimulation with varying frequency (1- 250Hz) on both ischemic limbs (N=80) for 1 hour per day for 13 weeks. The absolute claudication distance was employed as serial outcome measure to assess maximal walking capacity at baseline and following the intervention. Statistical significant improvement was registered in mean absolute claudication distance (p= 0.000; Wilcoxon Signed Ranks test) at follow-up relative to baseline. |
Introduction
Peripheral artery disease (PAD) is a highly prevalent disease estimated to affect over 200 million people worldwide.1 It is defined as a partial or complete obstruction of arteries due to the development of atherosclerosis2 and can affect all arteries distal to the aortic bifurcation.3 The presence of lower-limb atherosclerosis significantly increases the risk of cardiovascular and non-cardiovascular-related death while the disease causes walking impairment that can lead to intermittent claudication.4 Patients with concomitant diabetes mellitus are considered particularly vulnerable as they carry a poorer prognosis than those with either disease alone.5,6
Evidence shows that claudicants have poorer abilities in daily tasks such as ambulation,7 reduced quality of life8 and have been associated with higher prevalence of depression.9 Furthermore, several studies have shown that poor walking time is an independent predictor of cardiovascular events and mortality in PAD patients.10,11
Guidelines on the management of patients with PAD recommend supervised exercise training as a first line therapy to improve claudication symptoms.12,13 Exercise training comes with a number of barriers particularly in the elderly population. The majority of studies advocate supervised exercise programs; however, the usefulness of unsupervised programs has not been well established.12 Factors such as motivation to exercise, osteoarthritis and psychosocial factors may preclude adherence to any form of exercise therapy.14,15 Patients with co-morbid disease such as congestive heart failure or chronic obstructive pulmonary disease may also be advised to avoid strenuous cardiovascular activities.
As a result, in this vulnerable population there is a clear lack of treatment options available. In this context, electrical stimulation (ES) technology has been proposed as a potential alternative or adjunct to traditional exercise.16-19 However, only a few studies have evaluated the effectiveness of this therapeutic measure in PAD patients.18-20 Such studies are either conducted on laboratory ischemic animal models while those actually conducted on human are few and far between.19-20 This paucity has contributed to uncertainty amongst health care professionals on the use of such a technology as part of a treatment plan.
The aim of this study was to provide further insights on electrical stimulation by investigating whether sustained calf-muscle electro-stimulation for a duration of 13 weeks results in measurable improvement in functional walking capacity in PAD patients having concomitant diabetes mellitus and claudication symptoms.
Methods
Ethical permission was sought and obtained from the University Research Ethics Committee prior to initiation of a prospective, one-group, pretest-posttest study design. All participants signed an informed consent prior to inclusion in the study after being provided with an information sheet in Maltese or English, depending on their preferred language. All investigations were carried out in accordance with the Declaration of Helsinki (2008). Participants were recruited randomly from a Mater Dei hospital vascular database of patients with the following inclusion criteria:
- Diabetes;
- PAD defined with an Ankle Brachial Pressure Index (ABPI) <0.9;
- Abnormal spectral waveforms on the dorsalis pedis and posterior tibial arteries on both legs and suffering from calf muscle intermittent claudication reproducible on a graded treadmill test.
Exclusion criteria were aimed to control confounding variables. These included patients with renal disease, medial artery calcification (ABPI, >1.3) and sensory or autonomic neuropathy. Patients on oral claudication therapy or who had impediments to treadmill exercise, including previous foot/ toe amputations and physical/ physiological reasons such as blindness, were also excluded.
Eligible subjects were initially assessed (pretest) to establish a baseline and followed up after 13 weeks of ES intervention (posttest) in a temperature and humidity controlled laboratory at the Faculty of Health Sciences, University of Malta. The resting ABPI and spectral Doppler waveforms of the posterior and dorsalis pedis artery were measured at baseline to confirm the presence of PAD in accordance with the inclusion criteria set in the study.
The absolute claudication distance (ACD) was employed as the primary outcome measure to evaluate the therapeutic effects of ES on claudication symptoms. The ACD is defined as the distance at which claudication becomes severe and forces the participant to stop21 and was acquired using a graded treadmill protocol.22-23 The treadmill was initiated and maintained at a fixed speed of 3.2km/h while the treadmill grade was gradually increased by 2 degrees every 2 minutes up to a maximum of 10 degrees from an initial inclination of 0 degrees in accordance with the literature.24
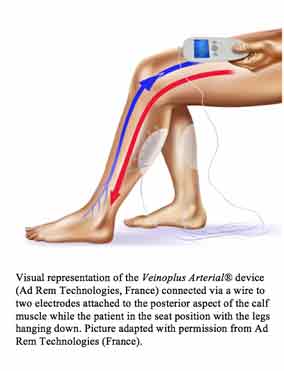
The Veinoplus Arterial model 2.1 (Ad Rem® Technologies, France) (figure 1) was used to generate the muscular contractions throughout the course of the intervention as per manufacturer’s instructions. This battery-operated device consists of a central unit with two adhesive electrodes attached transcutaneously on the calf muscle, generating the required electrical stimulation at varying frequencies (1-250Hz) through a series of rectangular pulses of low energy (<25uC) and low voltage (50V peak) within a fixed 1 hour session.
Following a demonstration session, recruited participants were given written instructions and log sheets to record daily use. Participants were instructed to use the device at any time of the day for 13 consecutive weeks in the seated position with the legs hanging down, manually and gradually increasing the intensity of the stimulation from the control unit along the intervention period. The optimal intensity of stimulation was set manually at the beginning of each session by the participants and was defined as the point at which a visible but comfortable calf contraction occurred on both limbs.
At the end of the 13 week period, participants were re-assessed under the same baseline laboratory conditions and utilizing the same treadmill protocol. Data was analyzed on IBM SPSS version 21. The Kolmogorov-Smirnov test revealed a non-normal distribution of the ACD data sets for both baseline and follow-up results. As a result, the Wilcoxon Signed Rank Test was used to evaluate for any significant differences in mean absolute claudication distance (ACD) at follow-up relative to baseline.
Results
From an initial assessment of 81 subjects, forty participants (30 males, 10 females; N=80 limbs) satisfied the inclusion criteria and were recruited in this study. At baseline, the cohort had a mean age 71 years (SD= 7); mean BMI 28.8 (SD= 3.7) and mean ABPI 0.70 (SD= 0.12).
The mean intervention period was 91.68 days (SD= 6.23) as quantified from the participant’s log-sheets. No evidence of non-compliance was reported while no subjects were lost to follow-up.
At baseline, the mean ACD registered was 333.71 meters (SD= 208). After 13 weeks of treatment the mean ACD was registered to be 470.7 meters (SD= 279). This translated in a mean improvement in the ACD of 137 meters (SD= 136), an improvement in maximum walking capacity of 41% relative to baseline that was found to be statistically significant (p= 0.000; Wilcoxon Signed Ranks Test).
Discussion
This study confirmed a significant improvement in maximal walking capacity on a treadmill in claudicants as evidenced by a mean increase (p=0.000) in the ACD of 137 meters following a consecutive period of 91.68 days (SD= 6.23) of 1 hour ES of the calf muscles per day.
The effects of ES on ischemic muscles is thought to include the augmentation of angiogenesis and morphological muscular adaptation.25-27 Studies have shown that ES augments the endogenous production of growth factors including vascular endothelial growth factor (VEGF) and expression of VEGF receptors such as fetal liver kinase 1 (FLK1), facilitating angiogenesis in ischemic muscle.25,28,29 The growth of new capillary networks within the ischemic muscle increases blood flow and oxygen availability to the exercising muscle, thereby lessening the ischemic symptoms.26 Additionally, muscle fiber activation is enhanced by ES, while selective recruitment of fatigue-resistant Type 1 muscle fibers is also thought to contribute to the improvement in claudication symptoms.26,27 These findings open up new opportunities of non-invasive treatment options for the claudicants population. Electrical stimulation has the potential of improving the functional walking capacity in claudicants with diabetes, thereby improving their outlook and quality of life. Furthermore, the ability of ES to produce muscular exercise activity without gross movement of joints or whole body exercise is an added advantage particularly in patients with co-morbid disease such as severe osteoarthritis, chronic heart failure or pulmonary diseases.
Thus ES should be considered as an adjunct treatment modality in order to improve walking capacity in symptomatic PAD patients living with Type 2 diabetes, particularly those who are impeded from undergoing vascular procedures, have already undergone these procedures but remain symptomatic and those who cannot perform exercise due to co-morbid disease.
It is recommended that a randomized controlled trial in a larger population is conducted in Malta with a view to strengthen the findings. This was not possible during this study due to ethical considerations regarding the use of placebo-controlled randomized trials and the inability to recruit an appropriately matched control group as a result of a limited number of available participants satisfying the inclusion-exclusion criteria. By evaluating the macro- and micro-circulatory response to ES, future studies may also reveal whether the effectiveness of ES of varying low to high frequencies may extend beyond improving muscular ischemic symptoms.
Conclusions
Electrical calf muscle stimulation significantly increased walking capacity in claudicants living with type 2 diabetes. ES should be considered as an adjunct treatment modality for claudicants who are precluded from following active physical exercise programs, such as the elderly, those with a lack of motivation to exercise, patients with arthritis and other physiological and psychosocial factors that make walking difficult.
Funding
The authors received no funding for performing this study. The intervention equipment was kindly supplied by Beta Pharma Ltd.
References
- Fowkes FGR, Rudan D, Rudan I, Aboyans, V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013 Oct 19; 382(9901): 1329- 1340.
- Omran M, Verma S, Lindsay FT. Suboptimal use of reduction therapy in peripheral arterial disease patients at a major teaching hospital. Ann Saudi Med 2011; 31: 371- 375.
- Bergiers S, Vaes B, Degryse J. To screen or not to screen for peripheral arterial disease in subjects aged 80 and over in primary health care: a cross-sectional analysis from the BELFRAIL study. BMC Fam Pract 2011; 12: 1-9.
- Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager, MA, Halperin, JL, et al. ACC/AHA 2005 Practice Guidelines for the Management of Patients with Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic). Circulation 2006 Mar 21; 113(11): e463- e465.
- Ogren M, Hedbland B, Engstrom G, Janzon L. Prevalence and prognostic significance of asymptomatic peripheral arterial disease in 68- year-old men with diabetes: results from the population study “Men born in 1914” from Malmo, Sweden. Eur J Vasc Endovasc Surg 2005; 29: 182 – 189.
- Mays RJ and Regensteiner JG. Therapy for peripheral artery disease: gaps in treating patients with claudication. Circulation 2014; 130: 929- 931.
- Gardner AW, Montgomery PS, Afaq A, Blevins SM. Patterns of ambulatory activity in subjects with and without intermittent claudication. J Vasc Surg 2007; 46: 1208–1214.
- Regensteiner JG, Hiatt WR, Coll JR, Criqui MH, Treat- Jacobson D, McDermott MM, et al. The impact of peripheral arterial disease on health-related quality of life in the Peripheral Arterial Disease Awareness, Risk, and Treatment: New Resources for Survival (PARTNERS) Program. Vasc Med. 2008 Feb;13 (1): 15–24.
- Smolderen KG, Hoeks SE, Pedersen SS, van Domburg RT, de Liefde II, Poldermans D. Lower-leg symptoms in peripheral arterial disease are associated with anxiety, depression, and anhedonia. Vasc Med. 2009 Nov;14(4): 297–304.
- McDermott MM, Guralnik JM, Ferrucci L, Tian L, Liu K, Liao Y, et al. Asymptomatic peripheral arterial disease is associated with more adverse lower extremity characteristics than intermittent claudication. Circulation. 2008 May 13; 117: 2484–2491.
- De Liefde II, Hoeks SE, Van Gestel YR, Klein J, Bax JJ, Verhagen HJ, et al. The prognostic value of impaired walking distance on long-term outcome in patients with known or suspected peripheral arterial disease. Eur J Vasc Endovasc Surg. 2009 Oct;38: 482–487.
- Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA Guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Apr 2;127(13):1425-43
- Conte MS, Pomposelli FB, Clair DG, Geraghty, PJ, McKinsey, JF, Mills JL, et al. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J Vasc Surg 2015 Mar;61(3 Suppl):2S-41S
- Oka RK, Altman M, Giacomini JC, Szuba A, Cooke JP. Exercise patterns and cardiovascular fitness of patients with peripheral arterial disease. J Vasc Nurs.2004 Dec;22(4):109-14.
- Cheetham DR, Burgess L, Ellis M, Williams A, Greenhalgh RM, Davies AH. Does supervised exercise offer adjuvant benefit over exercise advice alone for the treatment of intermittent claudication? A randomized trial. Eur J Vasc Endovasc Surg. 2004 Jan; 27(1): 17–23.
- Neuschwander TB, Macias BR, Hargens AR, Zhang Q. Mild external compression of the leg increases skin and muscle microvascular flow and muscle oxygenation during simulated venous hypertension. ISRN Vasc Med. 2012; 2012: 1-6.
- Banerjee P. Can electrical muscle stimulation of the legs produce cardiovascular exercise? J Clin Exp Cardiol. 2011; 2: 1-3.
- Abraham P, Mateus V, Bieuzen F, Ouedraogo N, Cisse F, Leftheriotis, G. Calf muscle stimulation with the Veinoplus device results in a significant increase in lower limb inflow without generating limb ischemia or pain in patients with peripheral artery disease. J Vasc Surg. 2013 Mar; 57(3): 714- 719.
- Anderson SI, Whatling P, Hudlicka O, Gosling P, Simms M, Brown MD. Chronic transcutaneous electrical stimulation of calf muscles improves functional capacity without inducing systemic inflammation in claudicants. Eur J Vasc Endovasc Surg. 2004: 27: 201-209.
- Presern- Strukelj M, Poredos P. The influence of electrostimulation on the circulation of the remaining leg in patients with one-sided amputation. Angiology. 53 (2002) 329-335.
- Jongert MWA, Hendriks HJM, Van HJ. KNGF-richtlijn Claudication Intermittens. Nederl Tijdschr Geneesk. 2003; 113: 3–58
- Kruidenier LM, Nicolai SPA, Willigendael EM, de Brie RA, Prins MH, Teijink JA. Functional claudication distance: a reliable and valid measurement to assess functional limitation in patients with intermittent claudication. BMC Cardiovasc Disord. 2009 Mar 2; 9:9: 1-7.
- Gardner AJ, Skinner JS, Canwell BW, Smith LK. Progressive vs single-stage treadmill test for evaluation of claudication. Med Sci Sports Exerc. 1991; 23: 402–408.
- Duprez D. Estimation of Walking distance and intermittent claudication: need for standardization. Clinical Perspective. Eur Heart J. 1999; 20: 641 – 644
- Hudlicka O, Brown MD. Adaptation of skeletal muscle microvasculature to increase or decrease blood flow: role of shear stress, nitric oxide and vascular endothelial growth factor. J Vasc Res. 2009; 46: 504- 512.
- Medeiros AH, Chalerge ST, de Carvalho CC. (2007). Muscle electrostimulation: alternative of adjuvant treatment to patients with peripheral arterial obstructive disease. J Vasc Bras. 2007; 6: 156- 162.
- Gregory, CM, Bickel CS. (2005). Recruitment patterns in human skeletal muscle during electrical stimulation. Phys Ther. 2005 Jan; 85: 358- 364.
- Kanno S, Oda N, Abe M, Saito S, Hori, K, Tabayashi, K, et al. Establishment of a simple and practical procedure applicable to therapeutic angiogenesis. Circulation. 1999 May 25;99(20): 2682–2687.
- Milkiewicz M, Hudlicka O, Verhaeg J. Differential expression of Flk-1 and Flt- 1 in rat skeletal muscle in response to chronic ischaemia: favourable effect of muscle activation. Clin. Sci. 2003; 105: 473- 482.