
Make Me More Compliant: The Oral Contraceptive Pill
Karl Cutajar
I n the 1930s the structure of steroids was discovered, together with the notion that high dose oestrogens, progesterones and androgens inhibited ovulation.1 Naturally, this has led to the development of oral hormonal contraceptives. This can be considered to be one of the epochal events of the 20th century since their direct and indirect effects on hormonal and metabolic pathways have shaped a new era of pharmacological control.
This research opened the doors to experimentation and development into an ideal oral contraceptive pill (OCP). The 1950s showed the introduction and marketing of the first combined OCP, Enovid® 10mg (Searle) (9.85 mg norethynodrel and 150 µg mestranol) for menstrual disorders. Following further stage 4 trials, the dose was decreased form a 10mg to a 2.5mg dose.1
Further studies and understanding of the steroid cycle and products led to the discovery of new progestogens and estrogens. This in turn led to the development of newer generation combined contraceptive pills
The evolution of the oral contraceptive pill ranged from changes in formulation, dosing, phases of action and active ingredient. The 1980s showed the introduction of the triphasic pills, whilst the 1990s showed the introduction of lower dose ethinylestradiol oral contraceptives focusing mainly on reduction of adverse side effects and enhancing tolerability to the combined oral contraceptive.1 In view of the decreased dosage and the 21/7 day regimes, this led to an increase in episodes of spotting or intracyclic bleeding leading to some women to shy away from the oral contraceptive or be less compliant, resulting in an increased number of unexpected pregnancies.2,3
The subsequent important milestone in the combined oral contraceptive pill development is the introduction of the 24/4 and 26/2 regimes.3,4,5 The shortening of the hormonefree interval resulted in further suppression of follicles and a decrease in spotting intervals, thus leading to better compliance which in turn translated in a decrease of unintended pregnancies.4
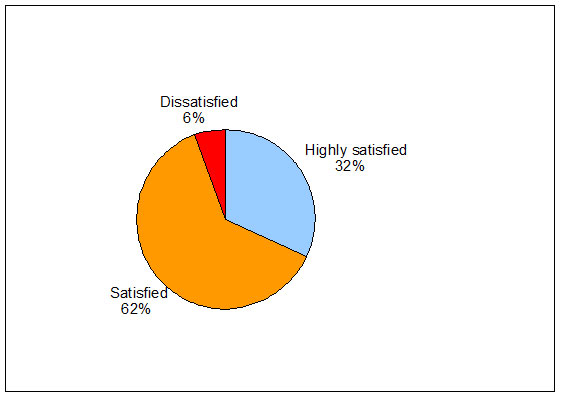
The various studies which have been conducted during the five years following the introduction of COCPs such as 3mg drosperenone and 0.02mg ethinylestradiol, 2.5mg nomegestrol and 1.5mg estradiol, and quadriphasic COCPs having a 24/4 regime have evidenced better compliance and tolerability.4,6,7 Benefits of a shorter hormone-free interval are that women do not experience hormonal withdrawal symptoms as intensely as women using 21/7 regimens. It has been demonstrated that women with a history of pre-menstrual dysphoric disorder experienced less premenstrual symptoms such as mood swings, water retention, bloating, headaches, acne and weight gain while taking a regimen of ethinyl-estradiol and droperinone/ normogestrol for a minimum of 24 out of 28 days.7,8 These benefits may translate to better user compliance and ultimately could reduce unintended pregnancy as shown in figure 1.9
In 2008, an ovulation inhibition study10 researched the effects of “missed pills” by replacement of the first three pills with a placebo after a completed cycle. It compared a 24-day with a 21-day regimen of 3mg drospirenone/0.02mg ethinyl estradiol. Results showed a suppression of ovarian activity, resulting in decreased hormonal fluctuations. This was substantially more pronounced in the regimen of 24 days of active tablets followed by 4 days of inactive tablets than the regimen of 21 days of active tablets followed by 7 days of inactive tablets.9 This means that the 24/4 regime is less prone to fluctuations especially if the patient misses a tablet.
Debate regarding the oral contraceptive pill still remains open with new regimes improving on the existing, in a struggle to create the “perfect” contraceptive with good tolerability and compliance with the least side-effects.
{kind=link}