
Management of localised renal cell cancer
by Pierre Vassallo – Renal cell cancer (RCC) is common, and its incidence is increasing due to increasing exposure to risk factors which include tobacco use, hypertension and obesity.
Localised renal cancers are often detected incidentally, and their increased incidence also results from the increased use of imaging. Localised renal cancer now accounts for 60-70% of new RCC cases. Many of these cancers are slow growing and show little tendency to metastasize.
Only a minority of patients with localised renal cell cancer have any clinical signs such as haematuria or abdominal pain. These tumours are often detected incidentally on ultrasound but are best characterised using computed tomography (CT),
where they may appear as a solid contrast-enhancing mass or a complex cystic lesion. Imaging features are similar on Magnetic Resonance Imaging (MRI) and the latter is equally accurate for the evaluation of renal lesions; it may be used in patients who are allergic to iodinated contrast material, in those with poor renal function, in lesions containing complex haemorrhage or where radiation exposure must be avoided (e.g. pregnancy).
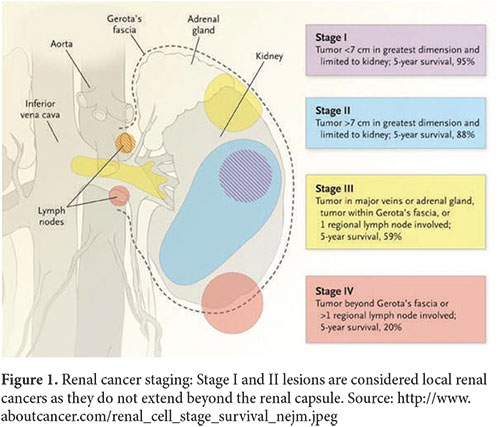
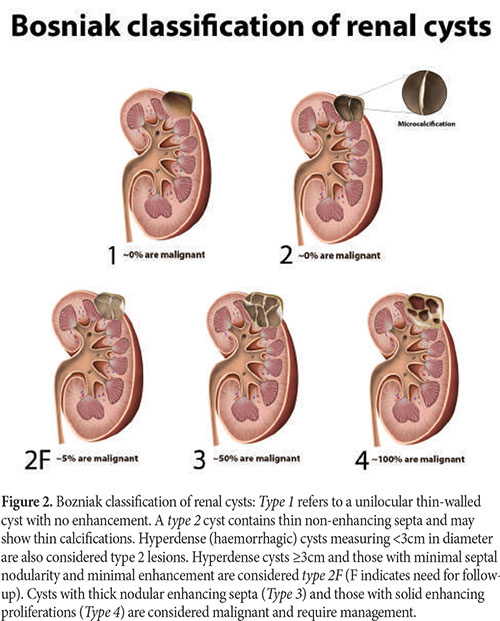
Localised renal cancer is defined as a stage I or II tumor that remains confined within the renal capsule (Fig 1). Since renal cancers may be cystic, it is important to identify those features in cystic lesions which point towards malignant disease. In 1986, Morton Bozniak suggested a classification of cystic lesions based on CT findings to help standardise their management (Fig 2). This cyst classification system has since then become widely accepted and is used to guide treatment decisions. Bosniak Type III and IV lesions are very likely malignant and require further management.
Management options for localised renal cancer include radical nephrectomy, partial nephrectomy, thermal ablation and active observation. The choice of treatment is individualised based on patient age and co-morbidities, tumor characteristics
and renal function considerations. A significant proportion of localised RCCs are indolent and slow growing; they can therefore be managed by nephron-sparing treatments (partial nephrectomy or thermal ablation) or even through active observation. The new American Urological Association (AUA) 2017 guidelines recommend a change in strategy with a decreased use of radical nephrectomy and an increased use of imaging-guided renal biopsy, thermal ablation and active observation.
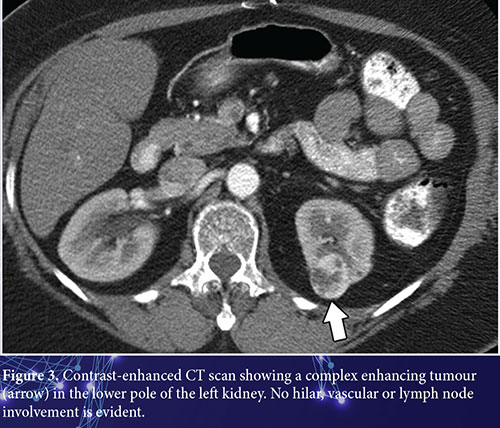
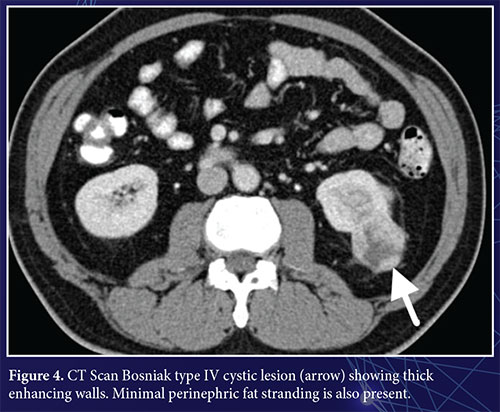
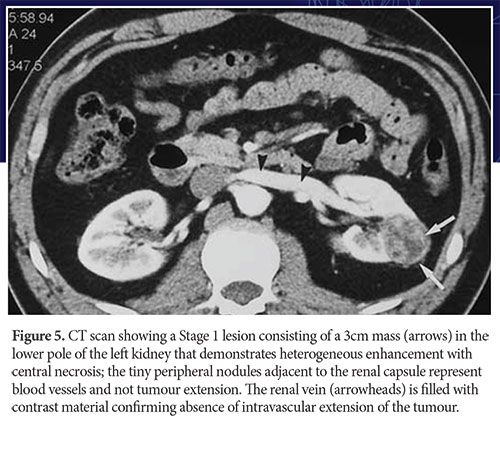
Radical nephrectomy is the preferred treatment in patients with aggressive tumor types, for larger tumours that show complex or infiltrative imaging features (Fig 3 and 4) and when normal contralateral renal function is present. Partial nephrectomy or tumour enucleation can be considered in tumours <4cm in diameter (Fig 5). These should also be considered in patients with an anatomical or functional solitary kidney, for bilateral or multifocal tumours, for patients with familial renal cell cancer, for young patients, and for those with limited renal function or with comorbidities that could lead to deterioration in renal function. In otherwise healthy individuals who present with a lesion that shows aggressive imaging features, a partial nephrectomy or enucleation is recommended without prior biopsy.
Imaging-guided tumour biopsy provides a means of confirming the diagnosis of malignancy and establishing the tumour subtype (and consequently the degree of aggressiveness of the tumour). In the past, it was claimed that percutaneous
biopsy was associated with an increased risk of tumor seeding along the biopsy tract. However, this is now known to be exceedingly rare particularly when using a coaxial technique; this technique allows multiple samples to be obtained and
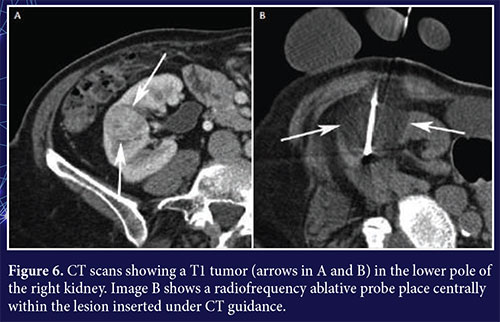
thermal ablation to be performed through a single tract. Thermal ablation can be a considered treatment option when nephron-sparing is a priority and in patients who are unfit for surgery. In patients who are frail, who suffer from multiple comorbidities or who refuse surgical intervention, and who have aggressive-looking lesions, biopsy and ablation may be performed in the same sitting. Tumour ablation is used for Stage 1 tumours and obtains most reliable results in tumours <3cm in diameter (Fig 6). Radiofrequency ablation or cryoablation may be implemented under imaging or laparoscopic guidance. Imaging guidance is more efficient that laparoscopic guidance and can be done under local anaesthesia. Imaging-guided core biopsy should always be performed prior to thermal ablation. Patients undergoing thermal ablation must be informed of an increased likelihood of persistence or recurrence of the tumour, which can be addressed by repeating the ablation.
In patients who are unfit for or unwilling to accept surgery and who have a non-aggressive appearing lesion, active observation with sequential imaging is advised. Active surveillance according to AUA guidelines should be used when anticipated risks of intervention or competing risks of death outweigh the potential benefits of active treatment. The said guidelines also state that active surveillance may be used as an initial management option in patients with suspicious lesions <2cm in diameter (Fig 7). However, the patient must clearly understand the risks of tumour growth and the importance of returning for a follow-up CT scan in 3-6 months. If lesion size increases to >3cm, if there is a growth rate of >5mm per year, or if there is an increase in tumour stage, a change in treatment strategy should be offered.
In summary, the current tendency is to move away from radical nephrectomy to nephron-sparing procedures for Stage 1 and 2 renal tumours. The increasing evidence that smaller tumours may be less aggressive or even indolent has changed recommended treatment protocols to favour more conservative surgery, thermal ablation or even active monitoring with imaging.
{kind=link}