
Spiral CT: The Gold Standard for Urinary Tract Stone Detection
by Pierre Vassallo
MD PhD FACA Artz fur Radiologie
Consultant Radiologist
In the past, the standard technique used for detecting urinary tract stones was the Intravenous Urogram (IVU). Limitations of this technique however, including non-radiographically opaque stones (15%), the use of potentially nephrotoxic intravenous contrast material (particularly in diabetics and patients with renal function impairment), and poor visualisation in obese patients and those with abundant intestinal gas, which have resulted in a considerable number of missed urinary tract stones.
Unenhanced spiral computed tomography (CT) has proved to be an accurate, safe and rapid examination used in the diagnosis and treatment of patients presenting with acute flank pain. During the past decade, unenhanced computed tomography has become the standard of reference in the detection of urinary calculi owing to its high sensitivity (>95%) and specificity (>98%) in this setting. Bowel cleansing, which is required prior to standard IVU and is frequently inadequate, is not necessary for unenhanced CT making it more comfortable for the patient and avoiding delays in the diagnostic process.
The spiral CT examination performed for suspected ureterolithiasis is conducted without intravenous or oral administration of contrast material. Because most ureteral stones are small, narrow collimation of 5mm is recommended. Most institutions perform helical CT with a pitch of 1, although there is no documented disadvantage to increasing the table speed. Multiplanar reconstructions are seldom necessary, but they can be used to illustrate stone location or other anatomic relationships.
Interpretation of the CT scans begins with inspection for secondary signs of urinary tract obstruction. The secondary signs of obstruction described, include asymmetric stranding of the perinephric fat, dilatation of the intrarenal collecting system, hydroureter, and unilateral renal enlargement (Figure 1). An extrarenal pelvis, a normal variant, should not be misinterpreted as a secondary sign of urolithiasis (Figure 2). The extrarenal pelvis is naturally wide and should not be mistaken for secondary widening due to obstruction and increased intrapelvic pressure; important distinguishing CT features include non-dilated calyces and a rapid tapering of the pelvis to a ureter of normal diameter. Unilateral absence of the white pyramid has been described as an additional secondary sign of an obstructing stone (Figure 3).
Further interpretation of CT scans involves following the ureters down to their insertion into the bladder. A thrombosed gonadal vein may occasionally be misinterpreted as an obstructed ureter, however meticulous inspection of each axial image in cine mode will allow the ureter to be followed throughout its course in most cases. Difficulty may be encountered in some cases due to paucity of retroperitoneal fat particularly in the pelvis where the ureter lies between bowel loops and the iliac vessels.
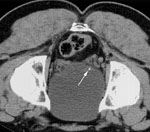
Phleboliths may also cause confusion, however they can generally be clarified by tracing the course of the ureter. The ureterovesical junction is often identified as a high-attenuation, thickened region in the midline of the posterior bladder wall (Figure 4). From this region, the distal ureter can be traced back, so that continuity of the calcification with the ureter can be either verified or excluded.
The soft-tissue rim sign can be used when the ureter cannot be confidently identified by any of the above methods (Figure 5); the ureteral wall around a passing stone is inflamed and appears as a thick rim around the stone. Although not all ureteral stones have this sign, approximately 77% of them are surrounded by a rim of soft tissue. Less than 10% of phleboliths have a soft-tissue rim.
Another pitfall may be encountered if a stone lies at the ureterovesical junction, as the tissue surrounding the stone may be so thin as to be imperceptible (Figure 6). This misleading appearance may lead to the conclusion that the stone has passed into the bladder. In such cases, rescanning the patient in the prone position helps one differentiate between passed stones that fall anteriorly and stones within the ureterovesical junction that do not.
Although virtually all stones previously considered radiolucent on plain radiographs, such as uric acid stones, are readily identified on CT scans, the recent use of protease inhibitors to treat HIV has led to an increasing prevalence of urinary tract obstruction caused by deposition of crystals that are nonopaque on CT scans. The presence of secondary signs of obstruction on the symptomatic side in the absence of an identifiable calculus typically prompts a differential diagnosis of a passed stone, pyelonephritis, or obstruction unrelated to stone disease. However, in a patient undergoing therapy with the protease inhibitor indinavir, the same constellation of findings should suggest the diagnosis of indinavir crystal deposition (Figure 7). Because demonstration of indinavir crystals requires gas chromatography, which is not available in most hospital laboratories, intravenous CT urography or retrograde urography should be used as they provide a rapid way to confirm the diagnosis of crystal deposition disease suspected on the basis of CT findings and clinical history.
Numerous diseases may manifest as acute flank pain and mimic urolithiasis. Up to one-third of unenhanced CT examinations performed because of flank pain may reveal unsuspected findings unrelated to stone disease, many of which can help explain the patient’s condition. Alternative diagnoses are most commonly related to gynaecologic conditions (especially adnexal masses) and nonstone genitourinary disease (example, pyelonephritis, renal neoplasm), closely followed by gastrointestinal disease (especially appendicitis and diverticulitis). Hepatobiliary, vascular, and musculoskeletal conditions may also be encountered. Vascular causes of acute flank pain (dissecting or leaking aortic aneurysm) must always be considered, since these constitute life-threatening emergencies that may require the intravenous administration of contrast material for diagnosis. Radiologists should be familiar with the typical findings of urinary stone disease at unenhanced CT, as well as the spectrum of alternative diagnoses that may be detected with this modality, to accurately diagnose the source of flank pain.
Figure Legends:

Figure 1. Axial CT scan shows stranding of the fat surrounding the left kidney and proximal left ureter (arrow heads). In addition, the left kidney is enlarged, with dilatation of the intrarenal collecting system (arrows).
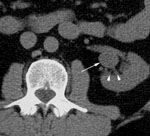
Figure 2. Extrarenal pelvis. (a) Axial CT scan shows apparent dilatation of the left renal pelvis (arrow), however note that the calyces are not dilated (arrow heads).
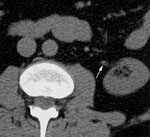
(b) Axial CT scan obtained at a slightly lower level shows that the extrarenal pelvis tapers rapidly to a normal proximal ureter that is not dilated (arrow).
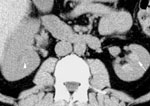
Figure 3. CT image reveals normal hyperdense pyramids in the left kidney (arrow) and isodense pyramids in the obstructed right kidney (arrow head).

Figure 4. Normal ureterovesical junctions. Axial CT scan shows bilateral hyperattenuating areas of focal thickening of the posterior bladder wall (arrows), an appearance that represents normal ureterovesical junctions.
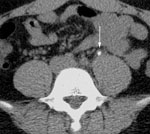
Figure 5. (a) Axial CT scan shows a rim of soft tissue surrounding a stone in the midportion of the left ureter (arrow).

(b) On an axial CT scan of a different patient, no soft tissue is present around a gonadal vein phlebolith. The normal left ureter was followed from above and identified as separate from the calcification (arrow).

Figure 6. (a) Axial CT scan of a patient with right flank pain, obtained with the patient supine, shows a stone adjacent to the right posterior bladder wall.
(b) On a scan obtained with the patient placed prone, the stone does not fall anteriorly, indicating the stone is still within the ureterovesical junction.
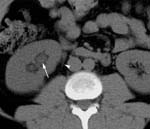
Figure 7. Protease inhibitor deposition in a 35-year-old man with HIV disease taking indinavir who presented with right flank pain radiating to the right groin. (a) Axial CT scan of the kidneys shows dilatation of the right renal collecting system (arrow) and mild stranding of the perinephric fat (arrow head) medial to the lower pole of the right kidney.

(b) A more inferior image shows dilatation of the right ureter (arrow).

(c) Another more inferior scan shows that the right ureter remains dilated to the ureterovesical junction (arrow). No calcification was identified.

(d) Subsequent retrograde ureterogram shows multiple filling defects in the distal right ureter. Stricture of the ureter distal to the indinavir fragments is likely caused by recent stone impaction near the ureterovesic