The Diabetic Foot – How to save a limb – Part II
by Kevin Cassar
What is the local situation?
The age standardized incidence rate of lower limb amputations in diabetics is 13.1 times (95% CI 9-17.2) greater than for the general population. The incidence of diabetes related lower limb amputations is 475 per 100,000 patient years or 10.2 per 100,000 patients per year.1 Extrapolating this to our own population, we would expect to have no more than 50 major amputations per year. If we take into account the higher prevalence of diabetes in our country we should not have more than 80 major amputations per year. As can be seen from figure 2, the number of major amputations per year in our country has been static at around 120 per year. Figure 3 shows that there is also a considerable number of minor amputations carried out per year, the numbers of which have again remained relatively stable in the past 5 years. Clearly the numbers performed locally are far in excess of those recorded in other countries. This begs the question of why our amputation rates are so high and what can we do to try and reduce this avoidable tragedy?
Foot screening
At present there is no national foot screening programme for diabetics. However the department of podiatry is working hard with the Health Care Services Division and Primary health to develop a national foot screening programme in the near future. This is crucial in our local context where the number of patients registered with a general practitioner or a general practice is a very small minority. Routine health checks and visits are also uncommon. Any investment in the development of such a programme would be well spent and would lead to a considerable reduction in amputations and probably overall costs.
Structured Foot Care
A multidisciplinary diabetic foot clinic operates from Mater Dei Hospital once weekly. This was set up in the last 2 years and provides a comprehensive service including education, podiatry, diabetes care, wound care and vascular surgery. There is also a daily diabetic podiatry service run by highly dedicated diabetic podiatrists who have direct access both to the diabetologists who work at the same clinic and to vascular surgery. Diabetic podiatrists regularly refer patients as emergencies as indicated.
Footwear, orthoses and total contact casting
Unfortunately there is only one orthotist to provide footwear and orthoses to the large number of diabetic patients, who is based at St Luke’s Hospital and therefore off-site. The number of patients requiring this service is high making it impossible for one person to provide an adequate service. Attempts are being made to develop this service and to make it more efficient and less reliant on overseas support. Attempts are being made to provide a pressure off-loading service within Mater Dei to provide adequate and effective off-loading for patients immediately after debridement or minor amputations. This will ensure that patients who are at high risk for further ulceration do not go on to develop further ulceration or gangrene in other toes of the same foot or the contralateral foot.
Arterial reconstruction
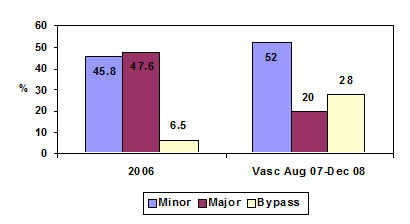
Recent improvements in imaging techniques and new equipment and personnel at Mater Dei Hospital has made the investigation of arterial disease more thorough and efficient. The advent of high quality CT angiography together with the acquisition of a high specification vascular ultrasound scanner has enabled increasingly more diabetic patients with arterial disease to be diagnosed and treated. Indeed there have been significant changes in the proportions of amputations and revascularisations done between 2006 and the present (Figure 4). The number of infrainguinal bypass procedures has also increased dramatically and in particular the number of femoro-distal bypasses has also increased. This indicates that increasingly more patients with diabetes are benefiting from revascularisation which has already translated into a reduction in the number of patients requiring major amputations.
How to save a limb
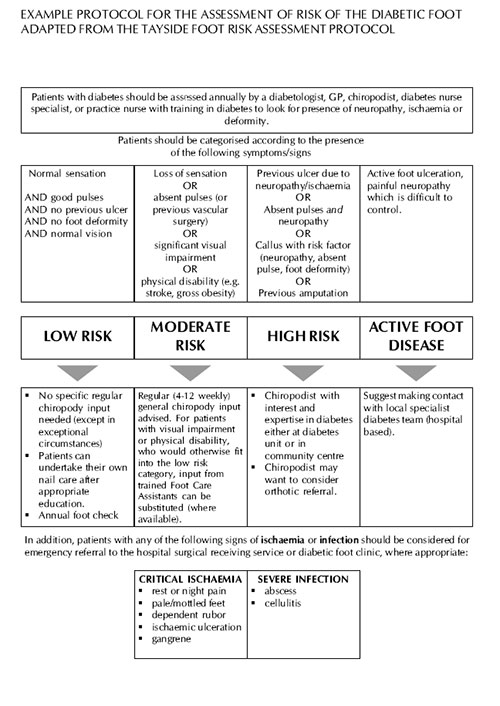
The family physician has a key role to play in this crusade to save limbs. Family physicians should themselves take the initiative to screen patients under their care with diabetes and categorise them into different risk groups and follow international guidelines as to diabetic foot care. Early referral to podiatry and diabetic podiatry according to the level of risk will have a determining effect on prevention of ulceration and limb loss. Most importantly however those patients with ulcerated feet or gangrene should be referred to the appropriate specialist as early as possible and those cases with features of critical ischaemia or severe infection should be referred as emergencies and seen within 24 hours. Risk factor control in those patients with diabetes and arterial disease will also contribute significantly to a reduction in morbidity and mortality in this group. Sadly we are still seeing considerable number of patients who are only referred once the limb is unsalvageable either through delayed presentation by the patient to the GP, or through misguided delay by the GP in an attempt to treat patients with ischaemic ulceration with local applications or dressings. It is also important for doctors working within accident and emergency departments to recognize the features of critical ischaemia and severe infection which warrant immediate hospital admission and treatment. Discharging these patients home on oral antibiotics without a proper vascular assessment and management plan is inadequate care. Finally we are all responsible for contributing to patient education. Intensive education has been shown to reduce amputations and recurrent ulceration in patients who have had previous diabetic foot disease.
Major amputations are associated with a 30 day mortality as high as 30%. The disability and reduction in quality of life associated with these procedures is considerable. Relatively small investments in education and prevention will mean not only less major amputations, but also less unnecessary deaths, improved quality of life for these individuals and dramatic reductions in health care costs.
References
1..New JP, McDowell D, Burns E, Young RJ. Problem of amputations in patients with newly diagnosed diabetes mellitus. Diabetes Medicine 1998: 15:760-4
Figure 2: Major amputations in Malta 2002-2009 (total number, above knee amputations and below knee amputations)
Figure 3: Minor amputations in Malta 2002-2009 (total, toe and transmetatarsal amputations)
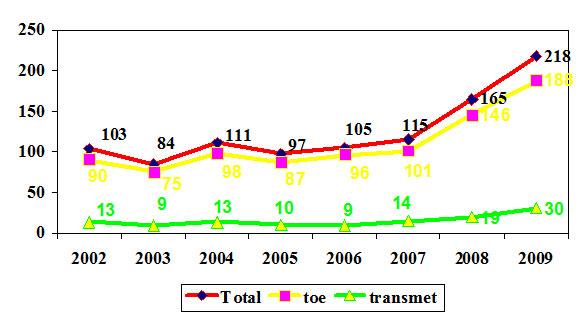
Figure 4: Proportion of Major/minor amputations/infrainguinal bypass surgery: comparison between 2006 and 2008 (the second group are patients treated by vascular surgery between August 2007 and December 2008 – these are the most recent figures; figures for 2009 not yet available)