Uncommon Inflammatory Breast Diseases that Mimic Cancer – Part 1
Dr Pierre Vassallo
Inflammatory breast lesions have radiologic features that often mimic those of malignancy. Infective mastitis is the most common condition that may be indistinguishable clinically from carcinomatous mastitis.
This article and the next one will present less common forms of inflammatory breast disease that is even more likely to constitute a diagnostic dilemma and require biopsy. The present article will present immunologic conditions causing inflammatory disease. The next article will discuss three categories of inflammatory disease: those caused by atypical infections, vascular disease and a further group in which the cause is unknown.
The immunological diseases discussed below include Churg-Strauss syndrome, amyloidosis, Wegener’s granulomatosis, sacroidosis and diabetic mastopathy. All closely mimic breast cancer in their clinical picture and radiographic findings.
Churg-Strauss syndrome
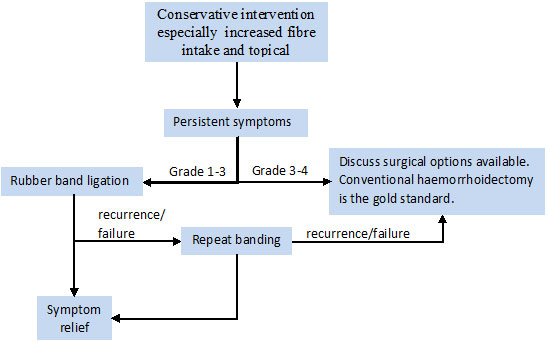
Churg-Strauss syndrome is a very uncommon condition characterized by asthma, pulmonary disease, eosinophilia, and necrotizing vasculitis. Its cause remains unknown, although the disease has classically been considered an immune/allergic disorder. Churg-Strauss syndrome almost invariably affects asthmatic patients. The histological features are vasculitis, tissue infiltration with eosinophils and extravascular granulomas, however these may not all be present concurrently. In 70% of cases there is lung involvement with transient patchy airspace consolidation (“infiltrates”) seen on chest X-rays and CT scans that usually lie peripherally. The heart and gastrointestinal tract are the next most commonly involved organs. Lymphadenopathy may be present. Breast involvement is rare. Mammographic features include diffuse increase in breast density (Fig 1) and skin thickening, both of which are also features of infectious mastitis and inflammatory carcinoma. Percutaneous biopsy (FNA or core biospy) may confirm the diagnosis by demonstrating vasculitis and eosinophilic infiltration and possibly extravascular granulomas.
Amyloidosis
Amyloidosis may be systemic and localized. In addition, it may be classified as primary, secondary, hereditary/familial, endocrine, and senile amyloidosis. Breast amyloidosis is rare and is usually accompanied by diffuse involvement of other organs. Histologically, amyloid deposition is seen (Congo Red stain) around ducts and blood vessels and within lobules that leads to atrophy and obliteration of these glandular components. Calcification and giant-cell reactions may also be present. Since amyloid may also be observed within breast cancer lesions, adequate histological evaluation with good tissue samples (i.e. not FNAs) is required to ensure the diagnosis.
Clinically, breast amyloidosis presents with a single nodule or multiple hard nodules. Mammographic findings include spiculated nodules, often accompanied by irregular or amorphous microcalcifications that may lead to a radiologic diagnosis of carcinoma (Fig 2). Amyloidosis in the breast may also present with clustered microcalcifications or diffuse breast infiltration with increased density and skin thickening, all of which are features associated with malignant disease.
Wegener’s granulomatosis
Wegener granulomatosis is a necrotizing granulomatous vasculitis that characteristically affects the upper and lower respiratory tracts and kidneys. The skin, joints and muscles, eyes, and peripheral nervous system are also often involved. Breast involvement is rare and is usually accompanied by diffuse systemic disease.
Clinical findings mimic those of breast cancer, but palpable tumors may be tender (unusual for cancer). Mammographically and sonographically, these lesions present with ill-defined masses that are indistinguishable from cancer (Fig 3). Biopsy is required to confirm the diagnosis. Histologically, there is usually a severe inflammatory reaction with numerous eosinophils and a prominent granulomatous component.
Sarcoidosis
Sarcoidosis is an immunologic disease that may affect the lungs, lymph nodes, skin, spleen, and liver. Breast involvement is very rare. It is seen as with other organ involvement, more commonly in women around the 3rd to 4th decade of life. Clinically, it presents with a hard mass that mimics cancer.
Sarcoidosis in the breast may present with intrinsic parenchymal involvement or with lymph node involvement. Histologically, it is characterised by clusters of epitheloid granulomas that from nodules along the lobules and ducts. Langhans’ multinucleate giant cells may for Schuamann bodies, but caseous necrosis, calcifications and lipoid necrosis are absent. A non-necrotising granulomatous sarcoid-like inflammatory reaction may be seen within a cancerous lesion and in tuberculosis.
On mammography, sacroidosis presents with an irregular, ill-defined or spiculated mass or even multiple small well-defined rounded masses, the latter is more common with lymph node involvement (Fig 4). Calcifications are absent.
Diabetic Mastopathy
Diabetic mastopathy presents with benign breast masses in women with long-standing insulin-dependent diabetes. Although generally considered a rare disease, it has been found in up to 13% of these patients and has also been reported in men. Diabetic mastopathy is characterized by a perilobar and perivascular lymphocytic infiltrate of mature B cells accompanied by intense keloidal fibrosis of the stroma with lobular atrophy and characteristic myofibroblastic epithelioid cells. Although fairly specific, these findings are also seen in a group of diseases grouped under the term lymphocytic mastopathy that has been seen in other immunologic diseases such as Hashimoto thyroiditis, Sjögren syndrome, and lupus erythematosus.
Clinically, diabetic mastopathy presents as single or multiple hard painless nodules that may be multicentric and bilateral. On mammography, these appear as ill-defined masses or as asymmetric breast density (Fig 5a). Ultrasound is more specific demonstrating a hypoechoic ill-defined mass with acoustic shadowing (Fig 5b). The latter is considered a very helpful sign and correlates with the extent of fibrosis; in early cases (with less fibrosis), this sign may be absent.
In summary, immunologic conditions may cause significant diagnostic difficulty in the breast, particularly since clinical, radiological and even some histopathological features overlap with those of cancer. The clinical history, radiologic signs and detailed pathological analysis are required to ensure a correct diagnosis. In addition, follow-up of these conditions is crucial to ensure lesion resolution with therapy.
Figure Legends


Fig 1: Known case of Churg-Strauss syndrome with a history of asthma, fever, purpuric cutaneous disease, tachycardia, lung disease, blood eosinophilia, and transbronchial biopsy confirmation. Initial mammogram (a) showed diffuse increased breast density with skin thickening (arrow) that diminished following treatment with corticosteroids (b).
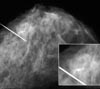
Fig 2: Amyloidosis in the breast. Mammogram shows an ill-defined lobular mass with microcalcifications and large calcifications.
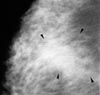
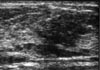
Fig 3: Wegener granulomatosis confirmed on core-needle biopsy. (a) Mammogram shows a suspicious focal asymmetric density (arrowheads). (b) Ultrasound image demonstrates an irregular hypoechoic mass.

Fig 4: Sarcoidosis presenting with a palpable mass. Systemic disease had been diagnosed 5 years earlier. A round mass with well-circumscribed margins in the outer part of the right breast.


Fig 5: Diabetic mastopathy in a case of long-standing insulin-dependent type 1 diabetes mellitus that presented with a palpable mass. (a) Mammogram shows subtle foci of asymmetric density laterally at the location of the palpable mass (arrows). (b) Ultrasound reveals an irregular hypoechoic mass with ill-defined margins and discrete acoustic shadowing.