
Imaging Hamstring Muscle Injuries
Pierre Vassallo
Hamstring muscle injuries (HMI) are the most commonly encountered sports-related injuries. There are also often quite difficult to treat. The aim of imaging such injuries is to provide an estimate of the nature and extent of the injury, which would guide treatment (conservative or surgical) and minimize unnecessary and often detrimental convalescence. Minimizing the duration of inactivity is not only important in professional athletes, but also in generally active individuals who enjoy sport for leisure.
The typical history of an HMI is sudden severe pain located in the posterior aspect of the thigh that usually stops further participation in the sporting activity. Not all pain in the posterior aspect of thigh is due to HMI; sciatic nerve root impingement and sacroiliac joint disease may result in a similar pain pattern.
The hamstring muscle group consists of three muscles: the biceps femoris, semitendinosus and semimembranosus muscles (Fig. 1).
The biceps femoris muscle has two heads (hence the name), the long head which attaches to the medial facet of the ischial tuberosity and the short head which attaches to the posterior aspect of the femur. The biceps femoris inserts distally into the head of the fibula, the lateral condyle of the tibia and the lateral fascia of the leg. Each of the two components of the biceps femoris has a different nerve supply, which may result in incoordination, a factor that has been attributed to its increased predisposition for injuries.
The semitendinosus muscle origin inserts in common with the long head of biceps into the ischial tuberosity (known as the conjoint tendon). It has a central raphe with superior and inferior muscle components and inserts distally in the postero-medial aspect of the tibia (Gerdy’s tubercle).
The semimembranosus muscle arises from the supero-lateral aspect of the ischial tuberosity, separate from the remaining hamstring muscle, and has a complex distal insertion composed of 5 variable bands, which attach to the medial aspect of the tibia, the adjacent knee joint capsule and associated posterior oblique and acruate ligaments. An additional variable attachment to the posterior horn of the medial meniscus may also be observed.
Since most of the components of the hamstring muscles cross two joints, the degree of stretching and tensile strength in these muscles is greater than muscles that cross single joints. The hamstring muscles are also mostly composed of Type 2 fibres, which have high tensile contractions and strength and are hence more prone to injury. Injures most commonly occur at the musculo-tendonous junction (MTJ), which is a 10-12cm transition zone that correlates with the transition of the myofibrils from the muscle into the tendon. Injuries may be of various degrees of severity, from a muscle ache that results from vigorous muscle exercise, through minor, moderate and severe strain to a complete tear. All forms of injury are related to a disruption of the myofibrils with resultant accumulation of extracellular fluid, which may be so minor that it is not detected on imaging studies. More severe degrees of myofibrillar disruption result in visible accumulation of extracellular fluid in the form of oedema. In the acute phase, haemorrhage may also be present at the site of injury. Subsequently, repair of the injury is through the laying down of fibrous tissue (scar), which may appear as early as 14 days after injury. Although scar tissue has considerable tensile strength, it results in shortening of the muscle as well as decreased muscle elasticity, both of which increase the risk of a future tear.
The most serious form of HMI is the proximal avulsion. This usually involves the common insertion and in adults does not involve bone (Fig. 2). In adolescents however, the apophysis is weaker than the musculo-tendonous structure and avulsion usually includes the bone. This type of injury is best assessed with MRI as the extent of the tear and tendon retraction are better visualised than ultrasound. In adolescents, the bony fragment is well seen on conventional X-rays (Fig. 3). Proximal avulsions of the hamstring muscles require immediate surgical repair. Distal avulsions of the individual hamstring muscle insertions may occur with ski and football injuries, but are much less common, with semitendinosus insertion avulsions (Fig. 4) being the most common. There is frequently evidence of prior damage to these distal tendons before the occurrence of a tear.
Partial hamstring tears (also known as strains) occur at the MTJ, and more commonly in the proximal MTJ particularly in the biceps femoris muscle. In this case, fluid and blood components lie between the intact myofibrils as they insert into the tendon of the muscle producing a feathered appearance of high signal on MRI (Fig. 5) and as a hypoechoic area on ultrasound (Fig. 6).
Tears may also occur at the junction between the muscle and its surrounding fascia. These are commonly known as epimysial fascial tears (Fig. 7). In contrast, intrasubstance tears present as blood and fluid collections within the muscle that show varying degrees of hyper- or hypointensity depending on the amount and state of the blood components present (Fig. 8). These tears are sometimes referred to as muscle belly tears. Scar tissue is seen on both MR and ultrasound imaging and may contribute to a re-tear of the hamstring muscles due to muscle shortening and diminished elasticity (Fig. 9).
There is a clear correlation between imaging findings and clinical outcome. Tear size is directly related to the number of days lost from competitive sport. Tears exceeding 50% of cross-sectional area of the muscle are associated with prolonged recovery period and most individuals will sustain a re-tear within 2 years. The degree of pain noted is also related to the size of the tear seen on MR imaging or ultrasound and is consequently also related to the length of recovery period. Individuals with clinical suggestion of a tear but no imaging findings show the best recovery rates. If there is imaging evidence of a muscle tear/strain in an athlete in whom this was not clinically suspected, it is advisable to suggest convalescence as continuing the sporting activity would likely lead to progression of the tear and a prolonged recovery period. In the early stages of injury, ultrasound and MR imaging have similar accuracy for lesion detection. In later stages (≥ 2weeks), when the extent of oedema has diminished, MR imaging is more accurate. Deep lesions (more common in muscular athletes) are better assessed with MR imaging. Epimysial injuries, which are more likely to be superficial, are better seen with ultrasound, while MTJ injuries that are generally more deeply located are better seen with MRI.
The importance of imaging findings when planning management of hamstring injuries cannot be understated. With increasing demands placed on athletes and increasing physical activity of the population in general, accurate advice on the management of HMIs is required and this can only be provided with accurate imaging.
Figure Legends
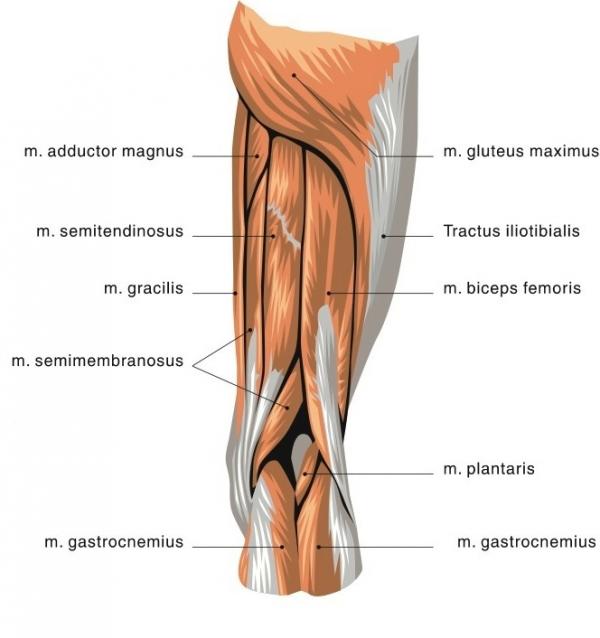
Fig 1. Anatomy of the hamstring muscles.
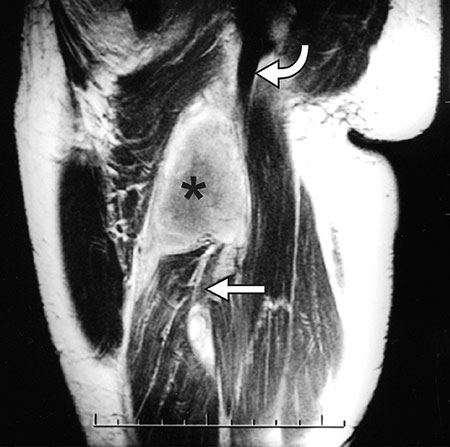
Fig 2. Proximal avulsion injury of the hamstring muscles. Oblique coronal T1-weighted MR image demonstrates a large hematoma (*) with retracted fibres of the semitendinosus muscle and the long head of the biceps femoris tendon (straight arrow). The semimembranosus muscle (curved arrow) is intact.

Fig 3. Bony avulsion (arrow) of the hamstring insertion seen on X-ray.

Fig 4. Coronal MR image shows avulsion of the semitendinosus tendon (arrow), with retraction of the muscle. The long head of the biceps femoris muscle is located laterally (*), with the semimembranosus muscle on the medial side.

Fig 5. Coronal oblique MR image shows a small region of hyperintensity in the biceps femoris (curved arrow), a finding that is consistent with oedema as a result of a subtle MTJ tear (straight arrow).
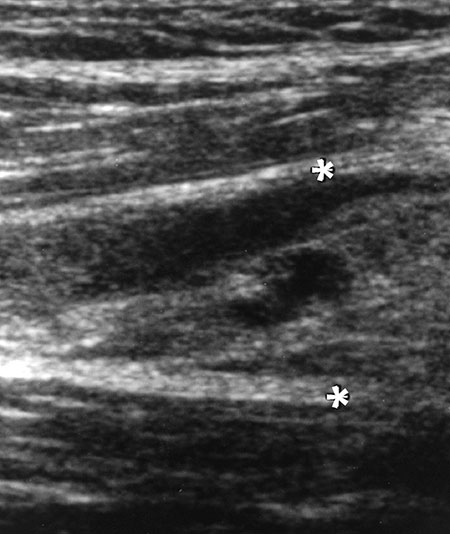
Fig 6. Longitudinal ultrasound image demonstrates a focal area of retraction (*) and hypoechogenicity consistent with a macroscopic tear in the distal MTJ of the semitendinosus.
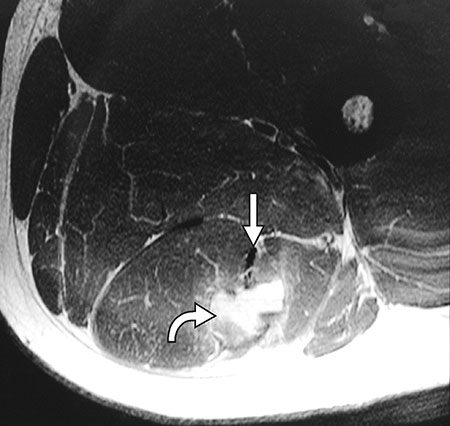
Fig 7. Epimysial fascial strain seen on axial MR image as an area of hyperintensity in the biceps femoris muscle (curved arrow). There is relatively little involvement near the tendon (straight arrow).
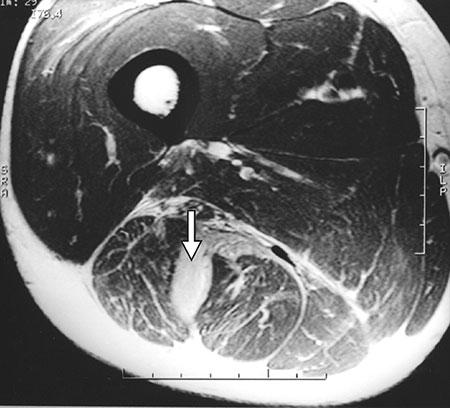
Fig 8. Muscle belly injury seen on axial proton-density–weighted MR image as an intramuscular hematoma in the biceps femoris muscle (arrow).

Fig 9. A re-torn semitendinosus muscle. MR image shows an area of hyperintensity (curved arrow) near the semitendinosus tendon (straight arrow) that is consistent with an MTJ tear. However, an irregular area of low signal intensity deep within the muscle (arrowhead) is characteristic of scar tissue following a prior myofascial tear. This may have contributed to the decrease in muscle elasticity ultimately leading to fresh tear.