
Imaging Pyelonephritis – Part I
by Pierre Vassallo MD PhD FACA Artz fur Radiologie
Consultant Radiologist
Urinary tract infections constitute a common cause for medical consultation and may occasionally require emergency admission to hospital. In adults, diagnosis of urinary tract infection is typically based on characteristic clinical features and abnormal laboratory values. Imaging is usually reserved for patients who do not respond to therapy, for those with recurrent infections and for those whose clinical presentation is either atypical or potentially life threatening.
Urinary tract infection typically originates in the urinary bladder (lower urinary tract); when it migrates to the kidney via the ureter or is seeded there haematogenously, a tubulointerstitial inflammatory reaction ensues, involving the renal pelvis and parenchyma. The condition is characterized as pyelonephritis.
Classic symptoms of pyelonephritis include an abrupt onset of chills, fever (temperature of 100°F or greater), and unilateral or bilateral flank pain with posterior costovertebral (“renal angle”) tenderness. These “upper tract signs” are often accompanied by dysuria and urinary frequency and urgency. Furthermore, acute pyelonephritis may cause gastrointestinal symptoms, such as abdominal pain, nausea, vomiting, and diarrhoea, which confound the diagnosis. Laboratory findings include pyuria, granular or leukocytic casts, bacteriuria, and a positive urine culture. Blood tests may show leukocytosis with a neutrophilic shift, elevated erythrocyte sedimentation rate, elevated C-reactive protein levels, and occasionally positive blood cultures that grow the same organism as cultured from the urine.
Immediately after the collection of urine for culture and antibiotic sensitivity testing, antibiotic therapy is started. Most patients respond successfully to antibiotics and do not require imaging studies or further intervention. In select clinical scenarios, however, diagnostic imaging plays a role, including (a) to assist in the diagnosis of acute pyelonephritis when the patient fails to respond to appropriate therapy within the first 72 hours (occurs in approximately 5% of patients), (b) to look for previously occult structural or functional abnormalities that may require intervention, (c) to assess those patients at significant risk for more severe life-threatening complications (eg, diabetic, elderly, or immunocompromised patients), (d) to characterize the severity of the infection to direct future therapy or interventions, and (e) to evaluate the extent of organ damage subsequent to a resolved acute infection. Pyelonephritis is but one form of interstitial nephritis. The most common organism causing UTIs is Escherichia coli.
The pathophysiology of acute, ascending pyelonephritis is best discussed as a continuum of disease. The bladder is originally inoculated with an infectious organism, which then migrates up the ureter to the central collecting system. This ascent occurs even in the absence of reflux, owing to special virulence properties of the bacteria, such as the adhesin P fimbriae and endotoxins. The endotoxins are believed to inhibit ureteral peristalsis by blocking the 
Abdominal radiographs were routinely obtained as the first component of an intravenous urogram, IVU; however, use of CT has overtaken that of radiography in nearly all institutions. The scout radiographs have been used in the past to detect urinary tract gas and calcifications, but pitfalls included unreliable differentiation of abdominal bowel gas from urinary tract gas and nonvisualization of small urinary tract calcifications overlying normal bony structures such as transverse processes. The IVU delineates the anatomy of the pelvi-caliceal system and provides an overview of the urothelial system from the kidneys to the urinary bladder. Findings seen in cases of acute kidney infections include renal enlargement, striated or delayed nephrograms (ie renal parenchymal enhancement), delayed caliceal appearance time, and dilatation or effacement of the collecting system. The weaknesses of excretory urography include the inability to characterize renal masses (ie, as cysts, neoplasms, or abscesses), the lack of fine parenchymal detail, and the dependency on functioning kidneys. In addition, several studies have demonstrated that only about 25% of patients with acute pyelonephritis have abnormal findings on an IVU. Therefore, more advanced imaging techniques are generally preferred. In addition, urinary tract stones that may accompany or cause pyelonephritis, are frequently only be visible on CT without IV contrast.
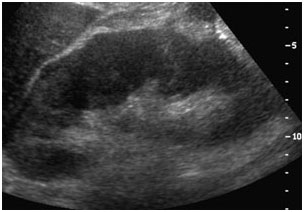
Ultrasonography (US) is frequently used as a first-line diagnostic tool to evaluate the urinary tract in patients with symptoms of pyelonephritis. Most patients with clinically suspected pyelonephritis have negative results from US, with several studies showing US abnormalities in only 24% of patients with pyelonephritis. US findings seen in pyelonephritis include congenital anomalies and a variety of changes in the renal parenchyma such as hydronephrosis, renal enlargement, loss of renal sinus fat due to oedema, changes in echogenicity due to both oedema (hypoechoic) or haemorrhage (hyperechoic) (Figure 2a), loss of corticomedullary differentiation, abscess formation, and areas of hypoperfusion (visible with power Doppler interrogation) (Figure 2b). Even when positive US findings are observed, US is limited in the definitive differentiation of calcification from intraparenchymal or collecting system gas, identification of perinephric extension of infection, and visualization of small microabscesses that are common in early acute infections (Figure 3). Occasionally, areas of abnormal echogenicity can have a tumour-like appearance (Figure 4). However, taking the clinical picture into consideration and if necessary short term US follow-up will resolve the issue in most cases.
Unenhanced CT is excellent for identifying urinary tract gas, calculi, haemorrhage, renal enlargement, inflammatory masses, and obstruction (Figure 5). Involved regions occasionally appear with lower attenuation related to oedema; less frequently, they have pockets of higher attenuation that are thought to represent haemorrhage (Figure 6).
When multiple round, peripheral hypoattenuation renal lesions are seen in the clinical setting of pyelonephritis, hematogenous seeding should be considered (Figure 7). Blood and urine cultures that grow organisms associated with skin or oral flora, such as Staphylococcus or Streptococcus species, support the hypothesis of hematogenous infection. However, when the lesions within the kidney or coalesce, differentiating between ascending and hematogenous infection may not be possible. Occasionally, these CT findings are identified in the absence of clinically suspected pyelonephritis and are mistaken for multiple neoplastic masses.
In addition to detecting and diagnosing nephritis more reliably, CT can monitor nephritis more accurately should the need arise (eg in patient’s not responding to treatment). However, follow-up is rarely required, as most uncomplicated cases will respond to first line treatment.
The next article will deal with complicated and less common types of pyelonephritis including xanthogranulomatous pyelonephritis, and tuberculosis, where CT is of even greater value.
Figure Legends

Figure 1. CT scan showing unilateral pyelitis in a patient with suspected acute bacterial pyelonephritis.
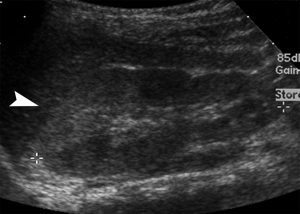
Figure 2. (a) US scan shows a wedge-shaped hyperechoic focus (arrowhead) in the upper pole of the right kidney related to acute bacterial pyelonephritis.
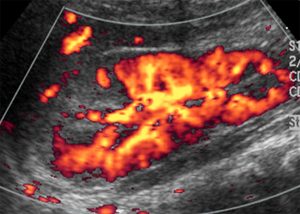
(b) Color flow US image demonstrates diminished flow through the involved area.
Figure 3.
(a) US image demonstrates a slightly enlarged right kidney that is otherwise unremarkable, belying the advanced disease.

(b) CT scan shows the enlarged kidney with multiple small low-attenuation foci from abscess pockets, findings that prompted nephrectomy.
Figure 4.

(a) US scan demonstrates a geographic, slightly lobulated “mass” (arrowhead) in the midpole of the left kidney, a finding that is suspicious for a solid tumour.

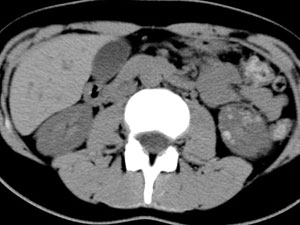
(b) CT scan shows multifocal regions of diminished enhancement that extend to the periphery of the kidney, findings consistent with interstitial nephritis.
Figure 5.

Unenhanced CT scan from a clinically documented case of acute bacterial pyelonephritis shows asymmetric enlargement and absence of the pyramids of the right kidney. The normal left kidney shows preserved pyramids [arrow].
Figure 6.
Unenhanced CT scan demonstrates multiple, scattered, round and oval hyperattenuation foci within the left kidney, findings indicative of hemorrhagic acute bacterial pyelonephritis.
Figure 7.

Acute bacterial pyelonephritis caused by haematologic seeding in a patient with Staphylococcus aureus endocarditis. CT scan demonstrates peripheral low-attenuation lesions (arrowheads) that are maturing into small abscess cavities. In such cases, blood and urine cultures grow the same organism.