
The new Death Certificate: Your role as Certifiers
by: Kathleen England MD, MSc (Public Health Medicine)
Medical Officer, Department of Health Information and Research
Information recorded on death certificates is used to produce population-based mortality statistics. Mortality data is used both in health monitoring and resource allocation as well as epidemiological research.
Although most doctors are confronted with the task of completing death certificates, many do not receive adequate training in this skill. Resulting inaccuracies in information undermine the quality of the data derived from death certificates (Myers et al., 1998).
Inaccuracies of death certificate information can occur as a result of errors at a number of the steps in the certification process. These include:
- Inadequate or misinterpreted clinical information can lead to erroneous ante mortem diagnosis, which are then recorded by the physician on the death certificate.
- Information can also be recorded wrongly on the death certificate due to lack of training in how to fill in death certificates.
- Modification of cause of death statement to avoid autopsy and distress to relatives.
- The final step in the process is coding of causes of death by a person who is usually trained. Studies have shown that this is relatively accurate and measures to improve coding and comparability between countries are being implemented.
During 2006-2007 the Department of Health Information and Research participated in an EU Project aimed at improving the quality of mortality statistics through improvements at certification and codification process depending on the individual needs of participating countries. This project led to the updating of the death certificate according to WHO and EU recommendations as well as the creation of training material aimed to assist certifiers in completing correctly the ‘cause of death’ section of the death certificate.
International form of the medical certificate for cause of death:
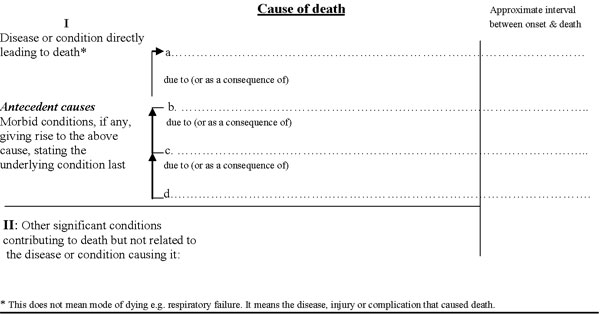
Part I of the certificate provides 4 lines, on which the sequences of events leading to death are recorded. The condition thought to be the underlying cause of death should appear on the last (lowest) completed line of part I and is usually the cause used in mortality statistics. If there is only one step in the chain of events, an entry on line I (a) is sufficient.
WHO defines the underlying cause of death (UCD) as: the disease or injury that initiated the train of morbid events leading directly to death, or the circumstances of the accident or violence that produced the fatal injury (WHO,1992).
An e.g. with 4 steps in the chain of events leading directly to death is:
- line a: Pulmonary embolism
- line b: Pathological fracture
- line c: Secondary carcinoma of femur
- line d: Carcinoma of breast ← (UCD)
Part II is for any other significant conditions that contributed to the fatal outcome, but were not related to the disease or condition directly causing death.
In a questionnaire sent to a number of doctors who are commonly involved in death certification they were asked to complete e.g.s of medical parts of death certificates. An number of frequent errors emerged:
- Major errors:
- Mechanism of death or non specific condition listed without an underlying cause e.g. cardiac arrest, respiratory failure. Because there could be hundreds of different causes leading to the same mechanism of death, this kind of description provides no useful information for cause of death statistics (Kircher et al., 1987) and therefore should not be used. The cause of non specific conditions such as heart failure should always be specified e.g. due to ischaemic heart disease.
- Improper sequencing e.g. underlying cause of death written on first line (line a) followed by other causes on subsequent lines.
- Competing causes: two or more causally unrelated, etiologically specific diseases listed in part I e.g. breast cancer, diabetes listed in part I.
- Not writing down method of injury e.g. not writing the fall as cause of a fractured femur.
- Limiting underlying cause of death to recent past. E.g. not taking account of the effects of a cerebrovascular accident 2 years previously.
- Minor errors:
- Absent time intervals
- Use of abbreviations.
Improving the quality of death certification:
Selection of a single underlying cause of death becomes more difficult in those who are older and have more morbid conditions. Diabetes mellitus presents a particular problem as this can be regarded as both an underlying cause of death giving rise to ischaemic heart disease and other complications, or it can be regarded as a contributing risk factor.
Training remains an important tool in improving the standard of the information written on death certificates.
Training tools available include:
- Training leaflet
- Training manual
- Web-based training tool
These can be accessed from the Department of Health Information and Research website on:
www.sahha.gov.mt/entities/healthinformation.html
The intended use of this package is to assist certifiers in providing quality information in areas where common problems occur by giving instructions and practical examples on the correct completion of the medical part of death certificates.
Medicine is becoming more and more evidence based. This increases the value of the information being collected, however it also emphasizes the need of more reliable data on which policy makers can base their decisions.
The attending physician is the one individual best able to prioritize the medical history to determine, in his or her best judgement, what disease process initiated the sequence of events leading to death (Kircher et al., 1987).
All information requested on the death certificate form should be written in a clear and legible manner. Abbreviations should not be used. All information regarding the deceased as requested on the death certificate should be completed.
References
:
Kircher T, Anderson RE. Proper completion of the death certificate. Journal of the American Medical Association 1987; 258: 349-52.
Myers KA, Farquhar D. Improving the accuracy of death certification. Canadian Medical Association Journal 1998; 158 (10).
World Health Organisation. Instruction Manual of the International Statistical Classification of Diseases and Related Health Problems, tenth revision, Geneva 1992.