
Impact of Social Determinants on Health in Malta
Michelle Deguara, Kathleen England, Natasha Azzopardi Muscat
Abstract
Socioeconomic conditions such as income and education have been demonstrated to be strong determinants of health status. This issue has been little researched in Malta and consequently has not made it to the top of the health policy agenda. This article reviews locally available evidence on the social determinants of health. Findings confirm that the inverse relationship between life-expectancy and chronic health conditions and lifestyle behaviours and socioeconomic status demonstrated in other countries, also exists in Malta. Greater awareness amongst health professionals and further research on the social determinants of health are necessary as rising income inequality and multi-ethnicity are both becoming important phenomena in Malta’s sociodemographic evolution. Public health approaches to tackle illness and wellbeing need to go beyond traditional educational campaigns and must focus on measures that support a more equitable and just society.
Introduction
The World Health Organisation (WHO) defines the social determinants of health as “the conditions in which people are born, grow, live, work and age. These circumstances are shaped by the distribution of money, power and resources at global, national and local levels.”1 Social determinants of health lead to health inequities which results in the unjust and unnecessary differences in the health status and health indicators of individuals.1 The difference in socioeconomic classes originate from people having different levels of education, income or occupation.2 Those who are in the lowest socioeconomic classes have high levels of ill-health, poor health indicators and also premature mortality.3 In 2015 the global life expectancy was 71.4 years (73.8 years for females and 69.1 years for males). The life expectancy varied by WHO region, with the WHO European Region having a life expectancy of 76.8 years whilst that of the WHO African region was 60 years.3 Apart from the variations in life expectancy and mortality rates between countries, disparities are also noted between different socioeconomic classes in the same country. In a study conducted by Mackenbach et al. comparing mortality rates between 22 European countries, it was noted that the social inequalities in mortality rates were smaller in Southern Mediterranean counties when compared to the inequalities in central and eastern Europe.4
Globally health researchers have been trying to study and analyse the disparities in health outcomes between socioeconomic groups and their causes. However, it is very challenging to highlight these differences to policy makers with a view to attempt to tackle and reduce these inequities and inequalities.5 The WHO’s Commission on the Social Determinants of Health, recommends three ways by which health equity can be tackled and improved:
· equitable distribution of resources, power and money;
· measurement and evaluation of the impact of policies on inequity;
· taking action on health equity.6
The Maltese scenario
In Malta there are various social benefits and social welfare services in place to try to bridge and minimise the gap between different socioeconomic classes and to reduce the impact of poverty. The 1970s saw the introduction of children’s allowances, a national minimum wage and the introduction of twothirds pension scheme. Also, in 1979 free hospitalisation was introduced as the first step towards the development of the National Health Service.7 Despite a generous welfare state, social inequalities still exist and according to the Statistics and Living Conditions survey carried out by the National Statistics office, the monetary at-risk-of-poverty rate stood at 16.3% or 68,658 individuals in 2015.8
The Maltese scenario In Malta there are various social benefits and social welfare services in place to try to bridge and minimise the gap between different socioeconomic classes and to reduce the impact of poverty. The 1970s saw the introduction of children’s allowances, a national minimum wage and the introduction of twothirds pension scheme. Also, in 1979 free hospitalisation was introduced as the first step towards the development of the National Health Service.7 Despite a generous welfare state, social inequalities still exist and according to the Statistics and Living Conditions survey carried out by the National Statistics office, the monetary at-risk-of-poverty rate stood at 16.3% or 68,658 individuals in 2015.8
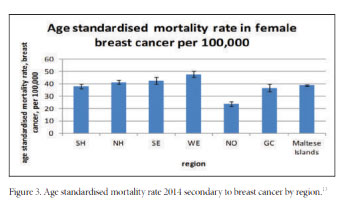
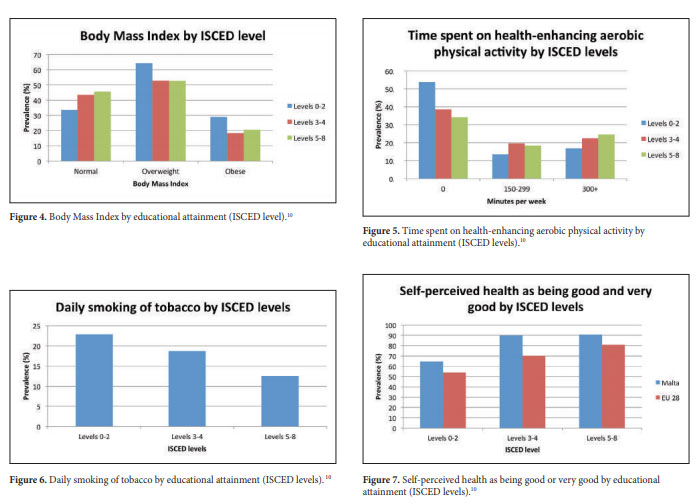
Analysis of cause-specific mortality may provide valuable insights on the source of health gaps observed between different socioeconomic groups. Regional analysis is sometimes used as a proxy for socioeconomic variables in the absence of more accurate indicators; however, regional differences may be the result of multiple factors and not only those related to socioeconomic classes. Figure 2 illustrates the age-standardised mortality rate due to circulatory diseases in Malta by region. The Western region, which is considered quite affluent,11 has the lowest agestandardised mortality rate for males. On the other hand the Western region has the highest mortality rate from breast cancer in females (Figure 3). Breast cancer incidence is known to increase with increasing affluence and socioeconomic status.12
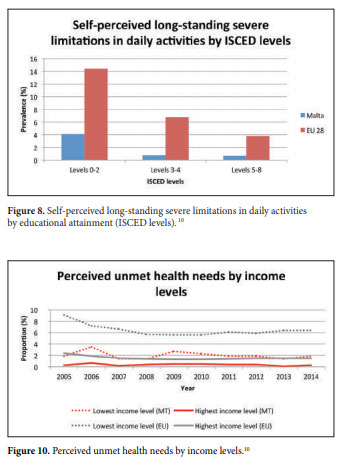
The inverse relationship between socioeconomic status and engaging in unhealthy behaviours such as unhealthy nutrition, lack of physical activity and smoking is well documented in literature.14 This high prevalence of unhealthy behaviours in individuals of lower socioeconomic status contributes further to inequalities in health.15 Results from the European Health Interview Survey (EHIS) carried out by the Directorate for Health Information and Research in 2014 highlight this inverse relationship; people with lower levels of education especially those of ISCED levels 0 to 2 have a higher prevalence of being overweight and obese, not engaging in any physical activity and smoking (Figures 4-6).10
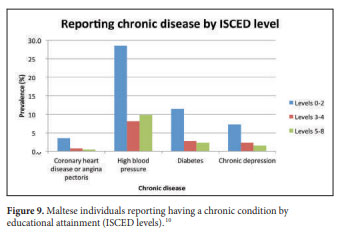
The way an individual perceives his or her own health status is also affected by socioeconomic determinants. In Malta and the EU, individuals with higher levels of education and higher income have a better perception of their health status (good or very good) (Figure 7). The perception of having a poor health may be related to the fact that people with lower levels of education report having more limitations in performing activities of daily living and also tend to suffer more from chronic diseases like coronary heart disease, hypertension, chronic depression and diabetes (Figure 8-9).
There is also an income gradient in relation to unmet health needs with those having lower incomes reporting a higher level of unmet health needs secondary to perceiving healthcare services as being too expensive, inaccessible or having long waiting times (Figure 10).10
Discussion and Conclusion
Over recent years many countries have improved the health status of their population but reducing the gap in health inequalities remains a challenge.2 As observed in the figures above, locally there is a gradient in the socioeconomic effect on health. As documented in the Marmot report16 reducing health inequalities due to socioeconomic factors needs to focus on reducing the ‘steepness of the social gradient on health’ with increased intensity for the most disadvantaged groups in society. The Marmot report also states that reducing health inequalities needs concerted effort at different domains such as education, employment and health and targeted approaches at different stages of a person’s life.16
At both EU and national level it is important that all policies which are developed factor in social determinants and their impact on health. In Malta the National Strategic Policy for Poverty Reduction and Social Inclusion 2014-2024 was launched in December 2014.17 The mission statement of this policy is “to provide a policy framework that promotes the well-being and improves the quality of life for all, particularly for persons at risk of poverty or social exclusion, based on the values of solidarity, equality, dignity and respect for fundamental human rights and social justice”. This policy acknowledges that everyone can be at risk of poverty and social exclusion but focuses more on the most vulnerable groups in the Maltese population: children, elderly, unemployed and working poor. The actions and objectives described in this strategy are aimed at preventing poverty and social exclusion and improving the socioeconomic status of everyone especially the vulnerable groups. The actions described the strategy also explore different ways of ensuring equal access to quality healthcare, strengthening primary health care and mental health services and reducing unmet health needs.17
There is a gap in local literature on the mechanisms involved in the relationships between socioeconomic status, unhealthy behaviours and poor health outcomes.14 Little is known about the effect that health promotion strategies have on different socioeconomic classes. If health promotion messages are more effective on people coming from higher socioeconomic classes and less effective on those coming from lower socioeconomic classes, they might be increasing the socioeconomic gap and health inequities. The reason for this may be that the health literacy in individuals with high socioeconomic status is higher than that of individuals having a low socioeconomic class.15
The results of the Health Literacy Survey commissioned by the Office of the Commissioner of Mental Health in 2014 concluded that 48.9% persons with no or primary level of education had poor health literary. The survey also found that low levels of health literacy were associated with low levels of self-perceived health.18 The need for further local research and monitoring of the socioeconomic effects on health is needed to highlight the impact that inequalities have on health outcome and to promote a more holistic approach to public health. Reducing health inequities is an ethical and socially just imperative.16
REFERENCES
1. World Health Organisation. Social determinants of Health [Internet]. [cited 2016 Nov 10]. Available from: http://www.who.int/social_ determinants/sdh_definition/en/
2. Mackenbach JP, Karanikolos M, Mckee M. The unequal health of Europeans : successes and failures of policies. Lancet [Internet]. Elsevier Ltd; 2013;381(9872):1125–34. Available from: http://dx.doi. org/10.1016/S0140-6736(12)62082-0
3. Commission on Social Determinants of Health, World Health Organisation. Closing the gap in a generation. 2008.
4. Mackenbach JP, Roskam A, Menvielle G, Kunst A. Socioeconomic Inequalities in Health in 22 European Countries. N Engl J Med. 2008;358(23).
5. The Lancet Global Health. Bridging the global health gap. Lancet Glob Heal [Internet]. The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license; 2016;4(9):e579. Available from: http://dx.doi.org/10.1016/S2214-109X(16)30190-5
6. Khanal P, Bhattarai N. Health beyond health to bridge the global health gap. Lancet Glob Heal [Internet]. The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license; 2016;4(11):e792. Available from: http://dx.doi.org/10.1016/S2214- 109X(16)30256-X
7. Camilleri R. A Demographic and Socio-Economic Profile of Ageing in Malta. International Institute on Ageing (United Nations – Malta); 1993.
8. National Statistics Office. Statistics on Income and Living Conditions 2015: Salient Indicators. 2016;1–9.
9. European Observatory on the Social Situation. Health Status and Living Conditions in an Enlarged Europe. 2005.
10. European Commission. Eurostat [Internet]. 2016 [cited 2016 Jan 2]. Available from: http://ec.europa.eu/eurostat/data/database
11. National Statistics Office. Statistics on Income and Living Conditions 2010: National Statistics Office 2012 https://nso.gov. mt/en/publicatons/Publications_by_Unit/Documents/C1_Living_ Conditions_and_Culture_Statistics/SILC_2010.pdf.
12. Robert S, Strombom I, Trentham-Dietz A, Hampton J, McElroy J, Newcomb P, et al. Socioeconomic risk factors for breast cancer: distinguishing individual- and community-level effects. Epidemiology. 2004;15(4):442–50.
13. Directorate for Health Information and Research. Mortality Register. 2016.
14. Pampel F, Kreuger P, Denney J. Socioeconomic Disparities in Health Behaviors. Annu Rev Sociol. 2011;(36):349–70.
15. Lenthe FJ Van, Bourdeaudhuij I De, Klepp K, Lien N, Moore L, Faggiano F, et al. Preventing socioeconomic inequalities in health behaviour in TEENAGE. 2009;10:1–10.
16. The Marmot Review Team. Fair society, healthy lives: strategic review of health inequalities in England post-2010. London: Marmot Review Team; 2010. 009;10:1–10.
17. Ministry for the Family and Social Solidaity. National Strategic Policy for Poverty Reduction and for social inclusion 2014-2024. Ministry for the Family and Social Solidarity http://mfss.gov.mt/en/ Documents/Poverty%20Strategy%2014%20English%20Version.pdf
18. Office of the Commissioner for Mental Health. Health Literacy Survey, Malta 2014. Compiled by the National Statistics Office on behalf of the Office of the Commissioner for Mental Health.