Inflammatory Bowel Disease – CT and MR Diagnosis
Pierre Vassallo
The term inflammatory bowel disease refers to two main entities, ulcerative colitis (UC) and Crohn’s disease (CD). The aetiology of these two conditions is uncertain. However, it has been suggested that they are the result of genetic factors leading to an abnormal immune response within the bowel wall to normal bowel contents. UC appears to precede CD in new cases. The incidence of IBD is increasing and there is a higher incidence of IBD in the developed world, which appears to suggest that a westernized diet may be a contributing risk factor.
Endoscopy is one of the main investigations used to diagnose inflammatory bowel disease. Two techniques are available, either conventional push endoscopy or capsule endoscopy. Push endoscopy has one major limitation in that most of the small intestine is inaccessible with this technique; the proximal jejunum and the terminal ileum may be accessible, but the intervening small bowel segments are not. One advantage of push endoscopy is that it allows lesion biopsy. Capsule endoscopy does visualize the whole bowel, but there is a significant risk of capsule retention particularly in the more severe cases of CD due to bowel strictures. Capsule endoscopy does not allow biopsy.
MR Enterography is a non-invasive imaging method that does not use ionizing radiation and that evaluates the whole GI tract. MR Enterography also depicts wall thickness and any extra intestinal manifestations of CD; it detects strictures, fistulae, mesenteric infiltration, lymphadenopathy and involvement of other organs. The detection of deep mural and extra intestinal manifestations and the presence of small bowel involvement are crucial in the distinction of CD from UC. If biopsy is deemed necessary, MR Enterography may help guide the endoscopist to the best location for biopsy. MR Enterography is valuable in assessing those bowel segments that are not accessible to endoscopy due to the presence of bowel strictures.
MR Enterography is performed using multiple imaging sequences including T2-weighted (Fig 1a), T1-weighted both before and after IV contrast administration (Fig 1b) and Diffusion Weighted Imaging (DWI) scans. Oral contrast material is given to outline the bowel wall one hour before starting the scan and IV medication is administered immediately before and during the exam to reduce bowel motility.
CD is a chronic relapsing/remitting inflammatory disease of the bowel that affects all bowel wall layers and can involve any part of the gastro-intestinal (GI) tract in a patchy multi-segmental fashion; this has led to the term skip lesions. The bowel segments most commonly involved by CD are the terminal ileum and the proximal colon. This contrasts with UC, which involves only the mucosal layer of the colon in one continuous segment. However, CD may occasionally involve only the colon.
The most common symptom of IBD is diarrhea. Abdominal pain, mild fever and weight loss may also occur. Overt GI bleeding is more common in UC than in CD; in CD, GI bleeding is usually occult and leads to anaemia. Clinical manifestations that occur with CD (but not UC) include perianal skin tags, fissures and abscesses, intestinal obstruction and extra-intestinal diseases in the skin, bile ducts, liver, bones and joints, eyes and kidneys.
The pathological changes seen in CD have been divided into four stages: acute inflammation, fistulisation/perforation, fibro-stenosis and reparative/regenerative stage. On MR Enterography, it is common to observe multiple (skip) lesions in different stages at any one time.
The earliest pathological finding of CD is the aphthous ulcer; this results from inflammation causing breakdown of the mucosal lining. It usually occurs over a lymphoid follicle and non-caseating granuloma formation may occur. Detection of these findings is key to reaching a histologic diagnosis of CD.
MR Enterographic findings of early CD include bowel wall thickening (>2mm for the small intestine and >3mm for the colon) with increased signal within the wall on T2-weighted images (Fig 2a). Contrast enhancement in T1-weighted images (Fig 2b and 3a) and diffusion restriction of DWI scans (Fig 3b) is seen within the inflamed segments of the bowel wall. Oedema of the bowel wall may result in bowel stenosis with intestinal obstruction; it is important to distinguish this from stenosis occurring due to fibro-stenosis as management differs. Obstruction due to acute inflammation is treated with anti-inflammatory medication (Fig 4), while that due to fibro-stenosis may require surgical intervention.
Fistulae and sinus tracts with abscess formation occur in around a third of patients with CD. A fistula may occur between two bowel loops or may occur to the skin or any other viscus such as the uterus, vagina or bladder. Endoscopy cannot assess the degree of the extraluminal extension. MR Enterography clearly depicts sinus and fistulous tracts (Fig 5) as well as any associated intra-abdominal abscess.
Intestinal stenosis due to fibro-stenotic disease is also readily detected by MR Enterography; a thickened intestinal wall with low T2 signal, moderate contrast enhancement on T1-w scans, no mesenteric infiltration or vasa recta enhancement and proximal intestinal dilatation are features of fibro-stenotic disease (Fig 6).
CD is associated with an increased incidence of colorectal cancer and lymphoma. Asymmetric thickening of the bowel, a mass-like lesion, non-response to treatment and enlarged mesenteric lymph nodes >1cm in diameter, should all raise the suspicion of malignant disease.
In contrast, UC is usually characterized by inflammation restricted to the mucosal layer of the colonic wall affecting one contiguous bowel segment. Occasionally, inflammation may extend into the distal ileum, a condition referred to as backwash ileitis. Characteristic MR Enterographic findings include sparing of the small intestine, wall thickening in the colon particularly the rectum and sigmoid colon with high T2 signal in the mucosal layer (Fig 7a) and contrast enhancement in the mucosal layer (Fig 7b) with no abnormality in the mesentery or the vasa recta.
Endoscopy will usually cover all diseased bowel in UC, however occasionally strictures impending scope entry may also occur. Strictures with UC need detailed investigation as colon-rectal cancer is also known to occur more commonly in these patients. MR Enterography is useful assess those unreachable segments of colon located proximal to a stenosis as well as to look for extra-colonic evidence of malignant disease.
In conclusion, endoscopy and MR Enterography are complementary examinations used in the diagnosis and management of IBD. They enable accurate characterization and classification of IBD in most patients and are extremely useful in guiding therapy of these conditions.
Figure Legends

Figure 1. a. Coronal T2-w image showing normal thin small intestinal bowel walls with low signal intensity (arrow).
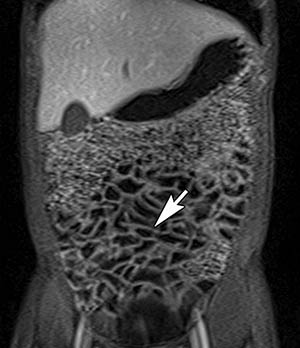
Figure 1b. Coronal contrast-enhanced T1-w scan showing normal thin uniformly-enhancing small bowel walls (arrow).
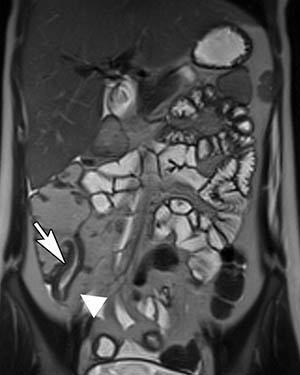
Figure 2. a. Coronal T2-w image shows thickening of the bowel wall (arrow) and proliferation of fat separating the bowel from adjacent segments (arrowhead).

Figure 2b. Coronal delayed post IV contrast T1-w image showing marked enhancement of the inflamed wall of the terminal ileum (arrow) with enhancement of the vasa recta (arrowhead) often referred to as the comb sign.
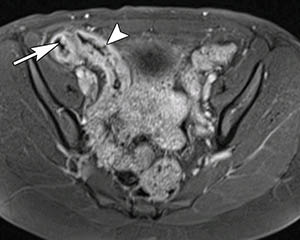
Figure 3. a. Transverse contrast enhanced T1-w image showing an enhancing terminal ileum with mucosal protrusions (arrow) and ulcerations (arrowhead).
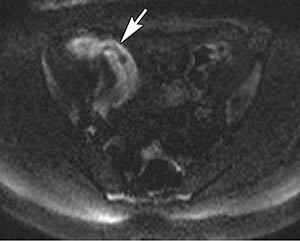
Figure 3b. Same case showing diffusion restriction on DWI as increased signal on high B-value image (arrow).

Figure 4. Transverse contrast enhanced T1-w image shows bowel wall thickening and enhancement (white arrow) and proximal bowel dilatation due to obstruction (black arrow).
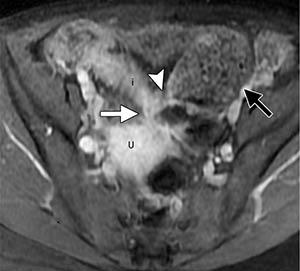
Figure 5. Transverse T1-w MR entrograph shows a fistula (white arrow) between the ileum (i) and uterus (U), a short-segment stricture (arrowhead) just proximal to the fistula and more proximal dilatation of the small bowel (black arrow).

Figure 6. a. Coronal T2-w MR Enterography shows wall thickening (arrow) with low signal at the site of ileo-colic anastomosis; the patient had undergone partial ileo-colectomy.
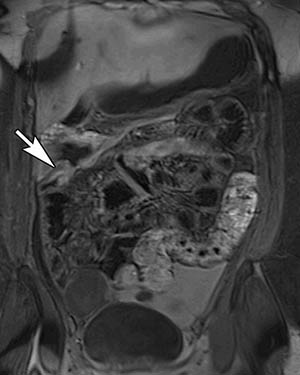
Figure 6.b. Coronal contrast enhanced T1-w image show only moderate wall enhancement (arrow) both no mesenteric infiltration or vasa recta enhancement indicative of a fibro-stenotic stage of CD.
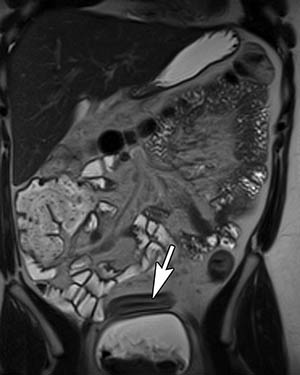
Figure 7. a. Coronal T2-w MR Enterography in a patient with UC shows sigmoid colonic wall thickening with high signal in the mucosal layer (arrow).

Figure 7.b. Coronal contrast enhanced T1-w image shows mucosal enhancement (arrow) but no involvement of the outer bowel wall, mesentery or vasa recta.