Imaging Pyelonephritis – Part II
by Pierre Vassallo MD PhD FACA Artz fur Radiologie
Consultant Radiologist
The last article introduced the clinical and radiological features of uncomplicated pyelonephritis, where the superior accuracy and efficiency of Computed Tomography (CT) over other imaging modalities was stressed. This article will briefly summarise the imaging findings of uncomplicated pyelonephritis and will discuss complicated and less common types of pyelonephritis including xanthogranulomatous pyelonephritis, and tuberculosis, where CT is of even greater value.
The recommended protocol for CT evaluation of pyelonephritis (or any other CT pathology) includes a three phase examination starting with a non-contrast-enhanced scan, followed by an contrast-enhanced scan performed 50-90 seconds after contrast injection and a delayed scan performed about 5 minutes after injection.
On unenhanced CT, regions of the kidney involved with pyelophritis may have lower density related to oedema and the kidney may be enlarged; less frequently, pockets of higher density may be present that are thought to represent hemorrhage. However, unenhanced CT may appear normal in pyelonephritis. Unenhanced CT is excellent for identifying urinary tract gas, calculi, hemorrhage and obstruction.
It is only after contrast material is administered that the diagnostic features of acute bacterial nephritis are revealed. After administration of contrast material, acute bacterial nephritis most commonly manifests as one or more wedge-shaped areas or streaky zones of lesser enhancement that extend from the papilla to the renal cortex. This pattern of differential enhancement reflects the underlying pathophysiology of tubular obstruction caused by inflammatory debris within the lumen, interstitial oedema, and vasospasm (figure 1). All three of these pathophysiologic disturbances tend to decrease the flow of contrast agent through the tubule. This explains why enhancement of the inflamed parenchymal areas is delayed and once contrast agent is delivered to the area the enhancement persists 3–6 hours after injection (figure 2). These foci of infection demonstrate reduced density during the early phase enhanced CT followed by increased density due to delayed clearance of the contrast agent as it slowly passes through the compromised tubules and collecting ducts.
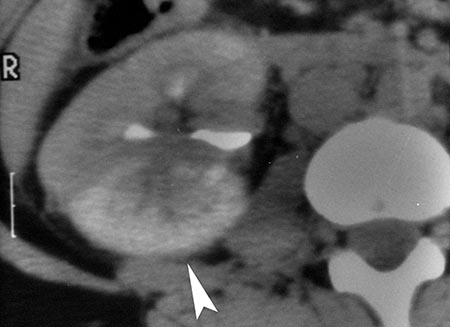
With more severe inflammatory disease, necrosis of renal parenchyma may occur with resulting abscess formation (figure 3). Abscesses may extend through the renal capsule outside the kidney to involve adjacent structures, most classically the psoas muscle. A renal abscess should be suspected when appropriate therapy does not lead to clinical response. Diabetic patients are predisposed to abscess formation, with 75% of all renal abscesses occurring in this patient population. Interestingly, up to 15%–20% of patients with an abscess have negative urine cultures. Abscess cavities may be visible on ultrasound (figure 4).
Infection is only one cause of interstitial nephritis. The inflammation can be induced by drugs, granulomatous diseases, metabolic disorders, and immunologically mediated mechanisms. These other entities are much less common than acute bacterial nephritis; thus, in the appropriate clinical setting, it is reasonable to assume that the characteristic findings of interstitial nephritis are caused by infection.
Chronic pyelonephritis is a somewhat controversial disease from a pathogenetic standpoint, as we are uncertain whether it represents an active chronic infection, multiple recurrent infections, or stable changes from a remote single infection; however whatever the pathogenesis, its radiologic appearance is the same. The imaging findings are characterized by renal scarring, atrophy and cortical thinning, hypertrophy of residual normal tissue (which may mimic a mass lesion), calyceal dilatation or clubbing secondary to retraction of the papilla from overlying scar, thickening and dilatation of the calyceal system, and overall renal asymmetry (figure 5). Hypertension is frequently a long-term sequela of chronic pyelonephritis.
Emphysematous pyelonephritis is a life-threatening necrotizing infection of the kidneys characterized by gas formation within or surrounding the kidneys (figure 6). The majority (approximately 90%) of patients have poorly controlled diabetes. Nondiabetic patients are typically either immunocompromised or have associated urinary tract obstruction secondary to stones, a neoplasm, or a sloughed papilla. The most commonly identified organisms are E coli, Klebsiella, and Proteus mirabilis. Without early therapeutic intervention, the condition rapidly progresses to fulminant sepsis, and carries a high mortality rate.
Emphysematous pyelitis is a less aggressive form of emphysematous infection of the upper urinary tract and is diagnosed when gas is localized to the renal collecting system (ie the ureter or renal pelvis). It is more common in women and is also associated with diabetes and urinary tract obstruction.
Pyonephrosis is simply an infected and obstructed collecting system, which frequently is be the result of calculi, tumors, complications from pyelonephritis (sloughed papilla), or strictures (figure 7). Early diagnosis is crucial because direct, immediate intervention is required with ultrasound guided nephrostomy to drain the obstructed renal pelvis and prevent decline in renal function and septic shock. Pyonephrosis should be suspected in any patient with a dilated renal collecting system and accompanying fever and flank pain.
Xanthogranulomatous pyelonephritis is a chronic destructive granulomatous process that is believed to result from an atypical, incomplete immune response to subacute bacterial infection. Most patients have no specific risk factors, although diabetes mellitus is seen in approximately 10% of patients. Female patients are more frequently affected than male patients in a ratio of 2:1, and the disease most commonly occurs in middle age. Symptoms are often nonspecific (low-grade fever and malaise), but flank pain and hematuria may help indicate a urinary tract problem. Pyuria and positive urine cultures are also frequently present.
In xanthogranulomatous pyelonephritis the renal parenchyma is ultimately replaced with lipid-laden (foamy) macrophages. Most cases occur in association with a renal pelvic calculus, and, consequently, hydronephrosis is thought to be a contributing factor. Ultimately, however, the loss of renal function and the destruction of the renal parenchyma are based on severe diffuse inflammation rather than obstruction. The most common organisms implicated are P mirabilis and E coli, but a variety of other bacteria may be found. The reason why in a small fraction of patients urinary tract infection progresses to xanthogranulomatous pyelonephritis is unknown. Without cross-sectional imaging, xanthogranulomatous pyelonephritis is difficult to detect. On plain X-rays, a large staghorn calculus may be seen, however this is not specific. Following contrast material injection, in an IVU, the affected kidney would show poor or no function which is also not specific. Ultrasound shows a dilated collecting system and calculi, which may be present in the absence of xanthogranulomatous pyelonephritis. CT contributes specific features that are diagnostic of this disease (figure 8); the affected kidney is enlarged, contains a large staghorn calculus and a collecting system distended with low attenuation material, which may have fat (rather than fluid) density. There is usually no renal parenchymal enhancement or function.
The increasing prevalence of tuberculosis in developed countries is well established and at least partly arises from both the spread of human immunodeficiency viral (HIV) infection and the continued emergence of mycobacterial strains with resistance to standard antibiotic therapy. The most common extrapulmonary site of tuberculosis is the urinary tract, with almost all cases resulting from hematogenous seeding. Despite the presumed route of spread from the lungs to the kidney, less than 50% of patients in whom urinary tract tuberculosis is ultimately diagnosed have abnormal results from chest radiography. Symptoms are often nonspecific (low-grade fever, malaise, or weakness). Hematuria and culture-negative pyuria may be seen at urinalysis.
After the tubercle bacilli reach the kidney, granulomas form and remain indolent for many years. If reactivation occurs, the infection spreads into the medulla, with direct involvement of the papillae. Further extension to the collecting system, with the potential for fibrosis, often occurs. Patients with untreated renal tuberculosis may totally lose renal function, and the disease may extend across retroperitoneal fascial planes to involve adjacent organs including the colon.
Imaging findings of renal tuberculosis result from the combination of papillary necrosis and parenchymal destruction. The latter typically involves the papillae initially, but cortical damage soon follows. The collecting system demonstrates thickening, ulceration, and fibrosis (often with stricture formation). The collecting system is distorted dilated calyces, strictures, sloughed or absent papillae and cavity formation, which arises from parenchymal necrosis, that may communicate with the collecting system (figure 9). In late stages, the whole kidney and ureter may be calcified.
This article has shortly reviewed uncomplicated pyelonephritis, which accounts for most cases of pyelonephritis. Complicated and less common forms of pyelonephritis have also been discussed. The importance of clinical data and frequently percutaneous imaging guided biopsy when interpreting CT images cannot be overstressed.
Figure Legends
Figure 1. (a) Acute bacterial nephritis seen in a resected kidney shows a wedge-shaped, lighter region of renal cortex that represents acute bacterial nephritis.
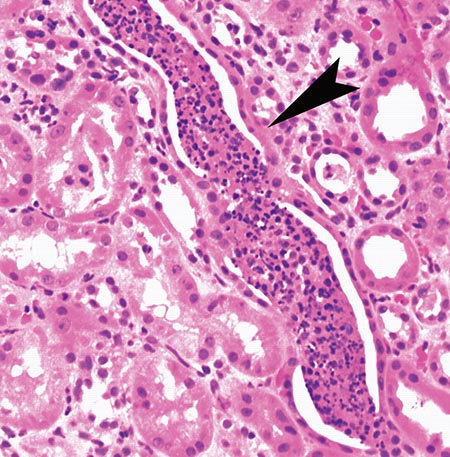
(b) Photomicrograph (original magnification, x400; hematoxylineosin stain) shows a collecting duct (arrowhead) filled with a cast of polymorphonuclear leukocytes.
Figure 2.

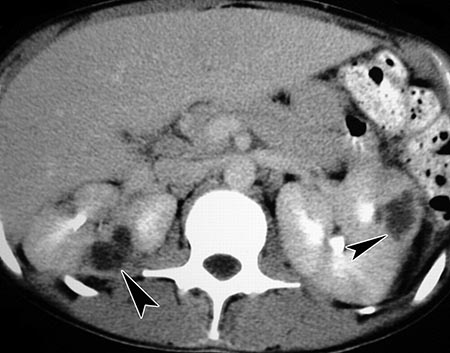
(a) Unenhanced CT scan showing enlargement of the infected right kidney and loss of medullary pyramids (note pyramids on normal left kidney (arrowhead)).

(b) Early enhanced CT scan showing area of diminished perfusion (arrow).
(c) Delayed scan (note contrast material is already in the renal calyces) showing an area of persistent contrast enhancement (arrowhead).
Figure 3.
(a) Enhanced CT showing multiple renal lesions with central fluid density representing abscesses.

(b) CT scan demonstrates an abscess cavity with a peripheral enhancing rim extending outside the right kidney and into the perinephric fat and psoas muscle.

Figure 4. Renal abscess cavity on ultrasound.
Figure 5.
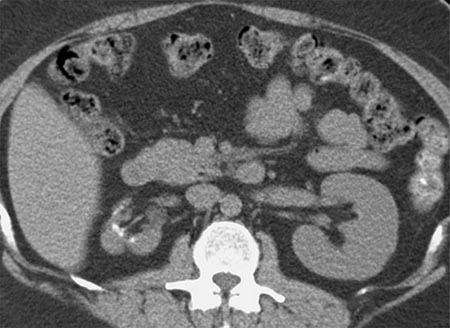
(a) Chronic pyelonephritis involving the right kidney, which is small, deformed right kidney with multiple deep scars and contains dystrophic calcifications.
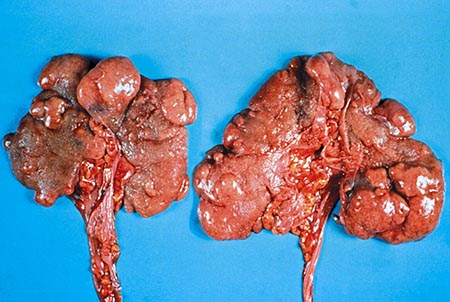
(b) Photograph of the resected kidneys demonstrates extensive bilateral scar formation.
Figure 6.

(a) Emphysematous pyelonephritis seen on plain abdominal X-ray showing lucent air that outlines both kidneys (arrowheads).

(b) Unenhanced CT showing gas bubbles (arrowheads) replacing the right kidney.

Figure 7. Pyonephrosis on ultrasound showing a dilated collecting system that is filled with echogenic debris (arrow) in a patient with fever and flank pain.

Figure 8. Xanthogranulomatous pyelonephritis on contrast-enhanced CT with bilateral staghorn calculi, with distension of the right collecting system secondary to inflammatory debris.
Figure 9.
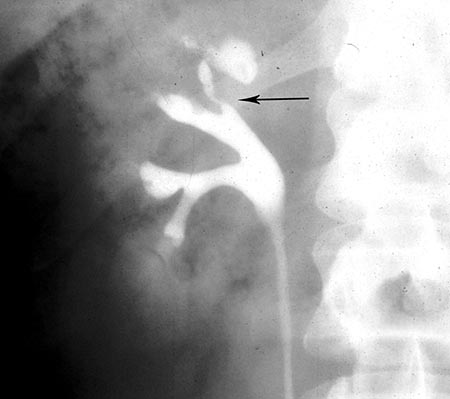
(a) Retrograde pyelogram in renal tuberculosis shows stenosis of the upper pole calyx (arrow) with associated papillary necrosis. The adjacent calyx is fibrotic and distorted.
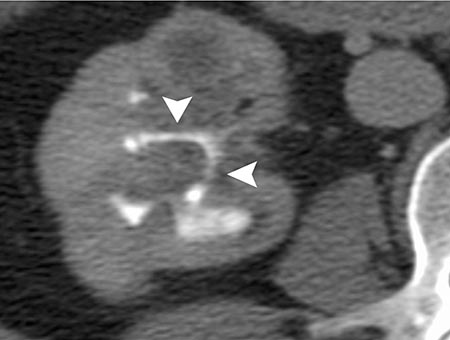
(b) Contrast-enhanced CT scan shows dilated calyces and narrowing of the infundibula (arrowheads).