
Polycystic Ovary Syndrome
MMSA
P olycystic ovarian syndrome (PCOS), previously referred to as Stein-Leventhal syndrome, is a worldwide disorder affecting about one fifth of women in their reproductive years1 . It causes disturbances in reproductive, endocrine and metabolic functions. PCOS is the focus of a great deal of research and studies indicate that its prevalence is on the increase2.
The main characteristics of PCOS are ovulatory dysfunction, hyperandrogenism, insulin resistance and obesity but one needs to investigate and exclude other functional disorders which may resemble PCOS. A key feature of the PCOS is an increased level of luteinizing hormone (LH) which may prevent the maturation of the ovum when it completes the first meiotic division and may thus be responsible for causing infertility in some women.
Diagnosis The European Society of Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM) state that in order for a woman to be diagnosed with PCOS, she must present with at least two criteria out of the following: ‘oligomenorrhea and/or anovulation, hyperandrogenism (clinical and/or biochemical) and polycystic ovaries, with the exclusion of other etiologies’3 .
Azziz4 states that the diagnosis of PCOS is essentially one of exclusion and that it can only be determined after ruling out thyroid dysfunction, androgen-secreting tumours and druginduced hyperandrogenism. The diagnosis consists of two principal steps:
1. Identifying features which suggest that PCOS may be present, such as:
• long-term menstrual dysfunction or irregularity
• hyperandrogenism, such as hirsutism, acne and alopecia
• polycystic ovaries (Figure 1)
2. Excluding related androgen excess of ovulatory disorders
Ovulatory dysfunction may result from thyroid dysfunction and patients with insulin resistance do not necessarily have PCOS. Patients with menstrual cycle disturbance and insulin resistance need to be examined for simultaneous signs of hyperandrogenism. The probability of having PCOS increases if a patient has polycystic ovaries together with ovulatory dysfunction with or without androgen excess.
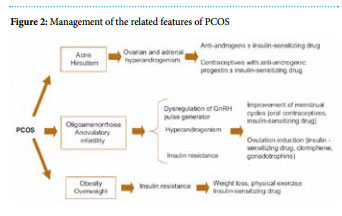
Treatment of PCOS is based on its underlying aetiology and on the presenting symptoms, as shown in Figure 2.
Conclusion
Research studies show that PCOS is not merely an endocrine disorder, but it also affects the hormonal, metabolic and psychosocial aspects which may have long-term consequences on the patient’s quality of life.
Apart from causing immediate morbidities such as chronic anovulation, menstrual irregularity and infertility during the reproductive years, PCOS may also precipitate psychological and emotional distress, cardiovascular disease and the metabolic syndrome, Type II diabetes mellitus as well as endometrial and ovarian cancer and therefore any woman with possible PCOS requires investigation and treatment.
References
1 Goodarzi M.O., Quinones M.J., AZZIZ R, et al. Polycystic ovary syndrome in Mexican Americans: prevalence and association with the severity of insulin resistance. J. Fertil steril 84, 766-9; 2005.
2 Balen A.H, Conway GS, Homburg R, Legro RS. Polycystic Ovary Syndrome A Guide to Clinical Management. Taylor & Francis Press London. (ISBN: Master e-book 0-0203-50615-4); 2005.
3 Fauser B, Tarlatzis B, Chang J, Azziz R et al. The Rotterdam ESHRE/ ASRM-sponsored PCOS consensus workshop group Revised consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS) J Hum Reprod 19, 41-47; 2004.
4 Azziz R. The Polycystic Ovary Syndrome; Current Concepts on Pathogenesis and Clinical Care. Springer Press New York (ISBN-13:978-0- 387-69246-3); 2007.